Selection of Approach
- Transperitoneal Approach:
- More Rapid Access (Best in Emergencies)
- Better Access to Right Renal Artery
- Better Access to Iliac/Femoral Arteries
- Retroperitoneal Approach:
- Better Access to Visceral & Supraceliac Aorta
- Better Access to Left Renal Artery
- Avoids Adhesions from Prior Operations
- Controversy if Equivalent or Lower Complications with Retroperitoneal Approach
Transperitoneal Approach
- Position: Supine & Arms Abducted
- Exposure:
- Midline Incision
- Retract Transverse Colon Cephalad
- Retract Small Bowel to the Right
- Divide the Ligament of Treitz & Retract Duodenum to the Right
- Incise Posterior Peritoneum from Ligament of Treitz Down to the Extent Necessary for Repair
- Angle to the Right of Aortic Midline to Avoid Injury to IMA
- If Suprarenal Clamp Needed – Open Posterior Peritoneum Up to the Level of the Renal Veins
- May Require Renal Vein Division (Divide Close to IVC to Allow Collateral Drainage Through Gonadal, Adrenal & Lumbar Veins)
- Repair:
- Systemic Heparinization
- Clamp Iliacs Distally & Proximal Aorta
- Distal First to Prevent Thrombus Embolization from Proximal Clamp)
- Incise an Aortotomy Longitudinally with a T-Shape on Either End
- Preform Proximal End-to-End Anastomosis
- First Clear Anastomotic Sites of Thrombus
- Clear Thrombus from the Aneurysmal Sac
- Preform Distal End-to-End Anastomoses
- First Clear Anastomotic Sites of Thrombus
- Allow Flushing of Graft & Back-Bleeding Before Completing the Anastomoses
- Closure:
- Achieve Hemostasis
- Close Aneurysmal Sac Over the Graft
- Close Posterior Peritoneum
- Use Omentum to Separate Graft from Bowel if Unable to Close Sac or Peritoneum
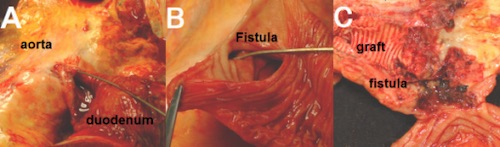
- Prevents Future Aortoenteric Fistula
- Close Abdominal Wall
Retroperitoneal Approach
- Position: Right Lateral Decubitus
- Exposure:
- Curved Skin Incision
- Start Along the 10th Intercostal Space at the Posterior Axillary Line
- Run onto the Abdomen Lateral to the Lateral Border of the Rectus Muscle
- Bluntly Dissect Peritoneum Off the Abdominal Wall
- Identify Left Psoas Muscle Retract Peritoneal/Retroperitoneal Contents Anteromedially
- Identify & Protect Left Ureter
- May Divide Left Diaphragmatic Crus to Better Access Supraceliac Aorta
- Repair:
- Systemic Heparinization
- Clamp Iliacs Distally & Proximal Aorta
- Distal First to Prevent Thrombus Embolization from Proximal Clamp)
- Incise an Aortotomy Longitudinally with a T-Shape on Either End
- Resect the Left Renal Artery with a Small Portion of Surrounding Aorta for Later
- May Preform Endarterectomy or Deploy Stent in Stenosed Celiac or SMA
- Preform Proximal End-to-End Anastomosis
- Proximal End Must Be Beveled to Include the Celiac, SMA and Right Renal Artery
- First Clear Anastomotic Sites of Thrombus
- Anastomose Left Renal Artery Back to a Side-Branch of the Graft
- Migrate Proximal Clamp Below the Renal Arteries to Minimize Ischemia Time
- Clear Thrombus from the Aneurysmal Sac
- Preform Distal End-to-End Anastomoses
- First Clear Anastomotic Sites of Thrombus
- Allow Flushing of Graft & Back-Bleeding Before Completing the Anastomoses
- Closure:
- Achieve Hemostasis
- Return Peritoneal Sac to Normal Configuration
- Close Abdominal Wall
Specific Vessel Considerations
- IMA Reimplantation Indications:
- SMA Stenosis
- Large IMA
- Backpressure < 40 mmHg (Poor Collaterals)
- Previous Colectomy (Risk Injury to Collaterals)
- Lumbar Arteries: