Focused Assessment with Sonography for Trauma (FAST)
- Rapid Bedside US to Evaluate for Free Intraperitoneal Fluid & Pericardial Effusion
- Use Curvilinear Probe
- Can Visualize ≥ 250 cc Fluid
- For ≥ 1 L Fluid 84% Sensitive & 71% Specific
- Windows:
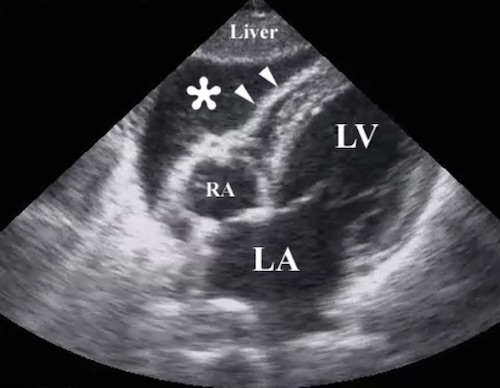
- Pericardial
- Should Be the First Area Viewed (Blood of Heart Allows Proper Gain Setting)
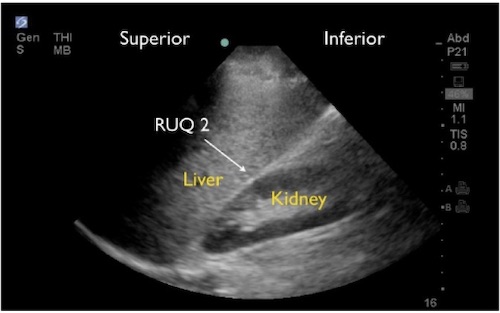
- Perihepatic (Morison’s Pouch)
- Most Sensitive Area for Free Intraperitoneal Fluid (Most Dependent Position When Supine)
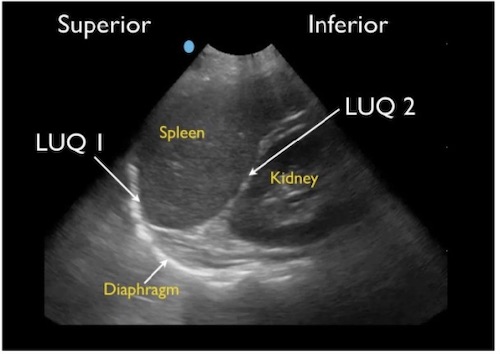
- Perisplenic
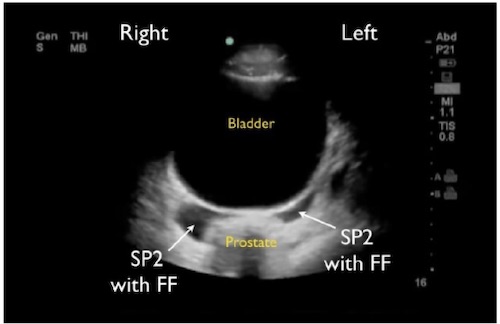
- Pelvic/Perivesicular
- Extended “E-FAST”
- Evaluates for Pneumothorax
- “Pleural Sliding” or “Comet Tail” Artifacts are Normally Seen – Lost in PTX