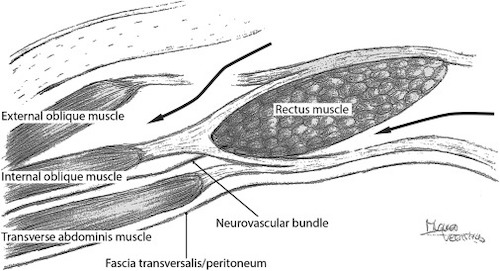
*Original PCS (Without TAR) Had Dissection Plane Between the Internal Oblique & Transversus Abdominis – Required Division of the Neurovascular Bundle with Denervation of Rectus Abdominis
Procedure
1. Incise the Dorsal Aspect of the Posterior Rectus Sheath 1 cm from the Medial Edge of the Rectus Muscle
Enter the Retrorectus Space & Dissect Laterally to the Semilunar Line
Care to Protect the Neurovascular Bundle Laterally Near the Semilunar Line
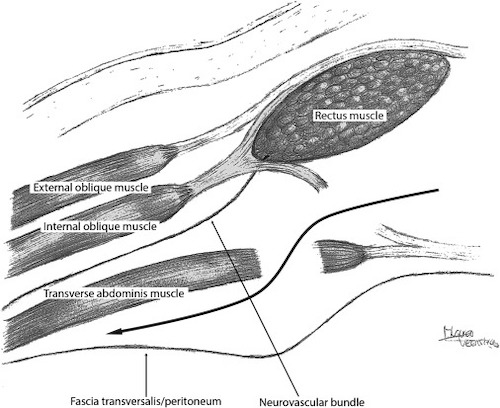
2. Incise the Ventral Aspect of the Posterior Rectus Sheath at Lateral-Most Edge
Exposes the Underlying Transversus Abdominis
Do Not Penetrate Through the Transversalis Fascia/Peritoneum
3. Dissect the Plane Laterally
Transversus Abdominis will be Anterior with the Transversalis Fascia/Peritoneum Posterior
Reconstruction
Reapproximate the Posterior Rectus Sheath to Midline
Typically Place a Sublay/Retrorectus Mesh
Reapproximate Anterior Rectus Sheath to Midline
Close Skin
Posterior Component Separation with TAR 1
Component Separation – Comparison & Complications
Comparison
Similar Recurrence Rate (< 10%)
Length Released is Debated
Some Report Similar Lengths
Many Feel ACS Allows More Medialization of the Fascia
PCS Mesh Extends Father Laterally – Preferred for Lateral Hernias or Ostomy
PCS Has Less Wound Complications – Does Not Require Large Subcutaneous Flap
Complications
Typically Have Improved Abdominal Wall Function
Surgical Site Infection
Most Common Complication
Seroma/Hematoma (2%)
Skin Flap Necrosis (1%)
Cause: Damage to Perforating Vessels
Iatrogenic Spigelian Hernia
References
Sneiders D, de Smet GHJ, den Hartog F, Verstoep L, Menon AG, Muysoms FE, Kleinrensink GJ, Lange JF. Medialization after combined anterior and posterior component separation in giant incisional hernia surgery, an anatomical study. Surgery. 2021 Dec;170(6):1749-1757. (License: CC BY-4.0)