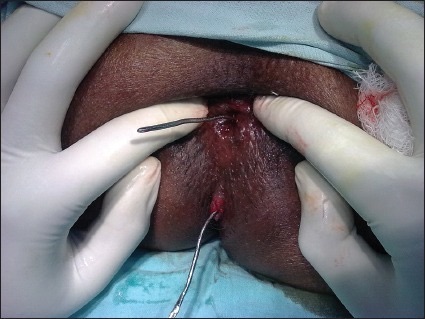
Incision and Drainage (I&D)
- Positioning:
- Bedside: Lateral Decubitus
- OR: Prone Jack-Knife
- Inject Local Anesthetic
- Incision Over the Abscess
- Semilunar or Cruciate (Cross)
- Oriented Radially
- Orient Over the Side Closest to the Anal Verge
- Not Over the Area of Greatest Fluctuance or Area Furthest from Verge
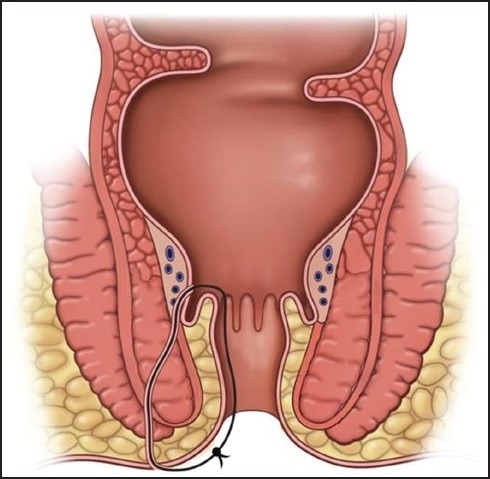
- Subsequent Fistula are Shorter and More Simple
- For Large Cavities (> 5 cm): Consider Ipsilateral Counter-Incisions to Avoid an Unnecessarily Large Single Incision
- Bluntly Probe the Cavity to Break All Loculations and Drain All Fluid Pockets
- Avoid Over-Aggressive Disruption – Risk for Sphincter or Pudendal Nerve Injury
- Finish Options:
- May Consider Packing with Daily Changes
- Most Common Although No High-Quality Evidence of Any Benefit
- Excise ≥ 1 cm Segment of Skin to Prevent Premature Closure without Packing