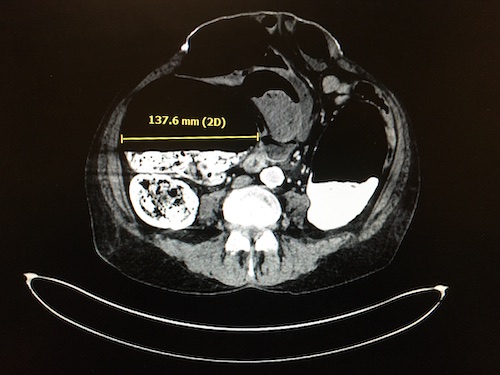
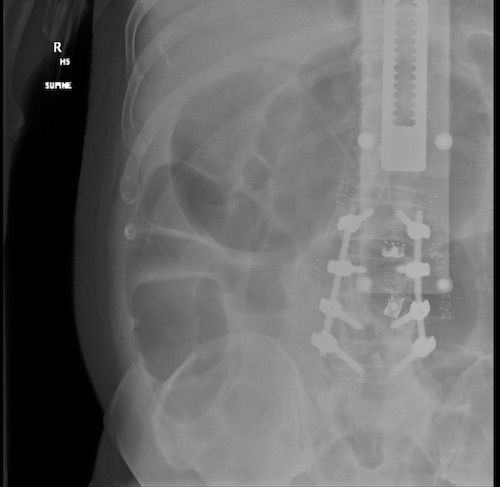
Large Intestine: Acute Colonic Pseudo-Obstruction (Ogilvie’s Syndrome) Acute Colonic Pseudo-Obstruction (Ogilvie’s Syndrome) BasicsAcute Colonic Dilation in the Absence of Mechanical ObstructionMortality Risk: 8%40-45% if PerforatedHigh-Risk for Perforation:Cecum > 10-12 cmDuration > 6 DaysRisk FactorsElderlyAcute Medical Illness – Infection or Cardiac Disease Most CommonOpiatesNonoperative TraumaSurgery – Cesarean Section & Hip Surgery Most CommonPresentationAbdominal Distention – Primary Clinical FeatureAbdominal PainNausea & VomitingDiarrhea or ConstipationDiagnosisDx: CTProximal Dilation Extending from the CecumExtends to:Hepatic Flexure: 17%Splenic Flexure: 56%Left Colon: 27%Can Monitor with Abdominal XR – Nonspecific for DxTreatment< 10-12 cm Diameter: Bowel RestSerial Abdominal Examination & Abdominal XRConsider Methylnaltrexone (Relistor) if Opiate-InducedGI Tract Specific Opioid Antagonist> 10-12 cm Diameter or Fails After 48-72 Hours: Neostigmine85-90% Success Rate*Monitor for BradycardiaIf Neostigmine Contraindicated or Fails: Endoscopic DecompressionMay Consider Second Dose of Neostigmine After 24 HoursConsider Leaving a Tube for Continued DecompressionIf Endoscopic Decompression Fails: Cecostomy TubeCan Be Performed by Colonoscopy, Interventional Radiology or SurgerySurgery Indications: Ischemia or Perforation Ogilvie’s Syndrome Ogilvie’s Syndrome