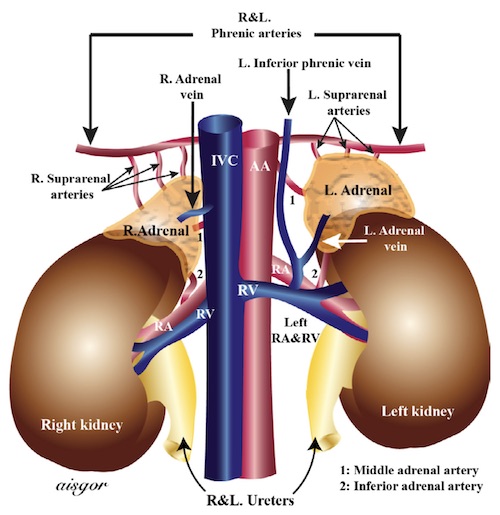
Adrenal Vasculature 1
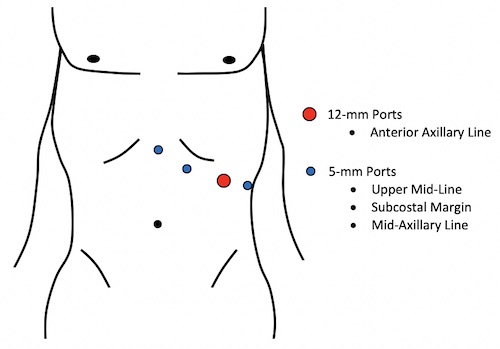
Left Adrenalectomy Port Placement
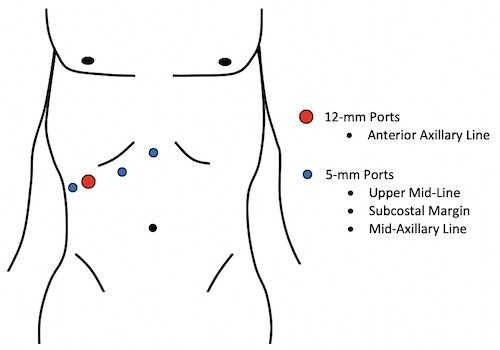
Right Adrenalectomy Port Placement
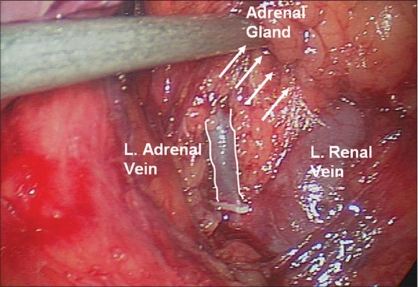
Left Adrenal Vein Draining into the Renal Vein 2
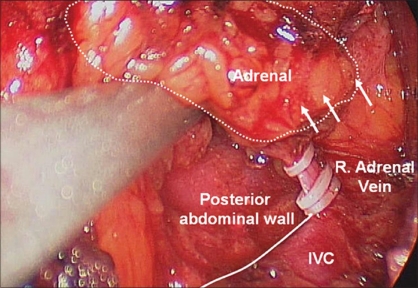
Right Adrenal Vein Draining into the IVC 2
Adrenal Vasculature 1
Left Adrenalectomy Port Placement
Right Adrenalectomy Port Placement
Left Adrenal Vein Draining into the Renal Vein 2
Right Adrenal Vein Draining into the IVC 2