Basics
- Largest Risk Factors: PAD & DM
- Should Generally Be Viewed as a Definitive Reconstructive Option, Not a Treatment Failure
Indications
- Acute Ischemia:
- Irreversible
- Severe with No Revascularization Options
- Failed Revascularization Attempts
- Chronic Ischemia:
- Failed Revascularization Attempts
- Severe with No Revascularization Options
- Severe Comorbidities
- Poor Functional Status
- Extensive Gangrene/Infection that is Not Salvageable
- Severe Infection Causing Pedal Sepsis
- Severe Traumatic Injury
- Malignancy
Amputation Staging
- Formal Amputation – Definitive Single-Stage Procedure
- Guillotine Amputation – Two-Stage Procedure
- First: Straight Amputation with Open Site
- Second: Formal Amputation a Few Days Later
Amputation Levels
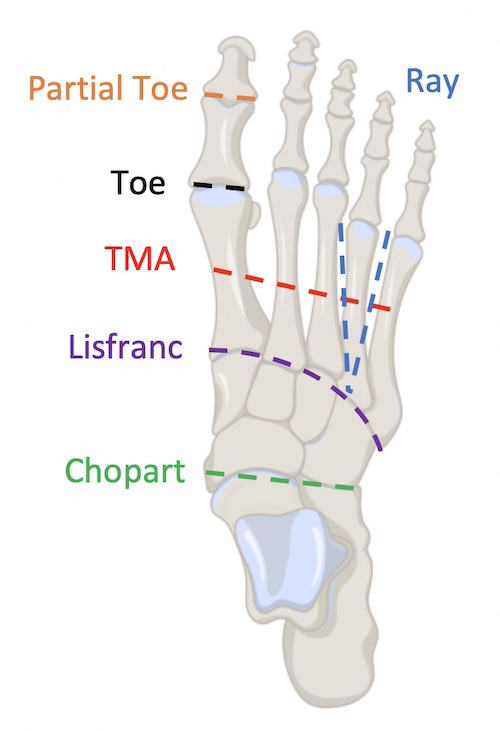
- Podiatric Procedures:
- Partial Toe Amputation – Part of a Toe
- Toe Amputation – Entire Toe
- Ray Amputation – Toe & Corresponding Metatarsal Bone
- Transmetatarsal Amputation (TMA) – Partial Foot Across the Metatarsal Bones
- Tarsometatarsal (Lisfranc) Amputation – Forefoot Amputation Across the Tarsometatarsal Line
- Midtarsal (Chopart) Amputation – Forefoot & Midfoot Amputation Sparing the Proximal Talus & Calcaneus
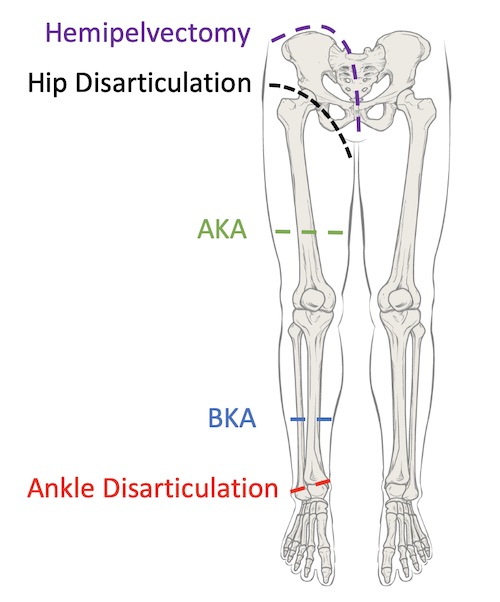
- Ankle Disarticulation (Syme’s Amputation) – Through Ankle Joint
- Major Leg Amputations:
- Transtibial – Below-Knee Amputation (BKA)
- Transfemoral – Above-Knee Amputation (AKA)
- Orthopedic Hip Procedures:
- Hip Disarticulation – Entire Leg
- Hemipelvectomy – Entire Leg & Ipsilateral Hemipelvis
Testing to Determine Site
- Objective Data Can Supplement but Not Replace Clinical Judgment
- Transcutaneous Oxygen (tcPO2)
- Generally Considered the Best Objective Test
- Sensor Placed on Skin, Heated to Decrease Flow Resistance & Oxygen Partial Pressure Measured
- Approximates True Arterial Oxygen Pressure at Questioned Site
- Values:
- < 16-20 mmHg: Likely to Fail
- ≥ 20-30 mmHg: Likely to Heal
- Other Less Reliable Objective Tests
- Skin Temperature – Not Reliable
- Ankle Brachial Index (ABI)
- Arteriography – Poor Correlation to Healing Potential