*Some Elect for Two Left Sided Ports Instead to Avoid Bladder Injury
Placement In Pregnancy
*Need to Avoid Gravid Uterus in Second & Third Trimesters
First Trimester
Normal Placement
Second Trimester
Access: Hasson (May Consider Veress at Subxiphoid or Left Costal Margin)
10 mm Port: Supraumbilical
5 mm Ports (x2): LLQ & RLQ
Third Trimester
Access: Hasson (Consider Veress Subxiphoid or Left Costal Margin)
10 mm Port: Supraumbilical
5 mm Ports (x2): Two Along Right Side
RLQ, Right Mid-Abdomen, RUQ or Subxiphoid
Also Consider Positioning in Full or Partial Left Lateral Decubitus During the Second/Third Trimesters
Basic Procedure
Laparoscopic Appendectomy
Position Supine, Left-Arm Tucked, Left-Side Down & Trendelenburg
Identify & Expose the Appendix Along its Length from Base to Tip
Bluntly Create a Tunnel Through the Mesoappendix at the Base
Staple Across the Mesoappendix Near the Appendix
Grey Staple Load (2.0 mm) Preferred – White Staple Load (2.5 mm) Has Significantly Higher Risk of Postoperative Bleeding
Staple Across the Base of the Appendix
Remove Appendix Through an Endoscopic Bag
Aspirate Overt Fluid but Avoid Peritoneal Irrigation (May Increase Risk of Abscess)
Close the Port Sites
Open Appendectomy
Incision Options:
McBurney’s Incision – Oblique Following Skin Lines
Center Incision at Site of Most Pain on Exam or at McBurney’s Point
Rockey-Davis Incision – Transverse Incision
If Converting from Laparoscopic: Low Midline Laparotomy (Connecting Periumbilical & Suprapubic Incisions
Using a Muscle Splitting Technique Dissect Through the Abdominal Wall
Locate the Ascending Colon/Cecum & Then Identify the Appendix
Mobilize Appendix into the Opening
Divide the Mesoappendix
Divide the Appendix at its Base
Close the Abdominal Wall & Incision
Laparoscopic Appendectomy 1
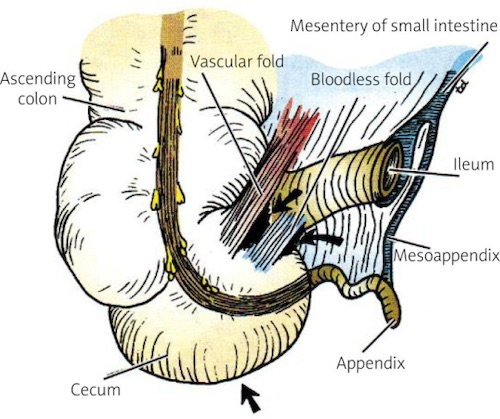
Appendix Anatomy 2
Complications
Surgical Site Infection
Most Common Complication
Laparoscopic Risk: 1.9-3.7%
Open Risk: 4.3-7.0%
Intraabdominal Abscess
Risk:
Overall: 2-4%
If Perforated: 6-10%
Higher Rates in Laparoscopic Than Open Surgery
Tx: Percutaneous Drainage
Stump Appendicitis
Recurrent Appendicitis Due to Incomplete Appendectomy Leaving an Excessively Long Stump
More Common After Perforation
Tx: Stump Resection
May Require Partial Cecectomy or Bowel Resection
Other Complications
Bleeding/Hematoma (1%)
Bowel Injury
Incisional Hernia
References
Strzałka M, Matyja M, Rembiasz K. Comparison of the results of laparoscopic appendectomies with application of different techniques for closure of the appendicular stump. World J Emerg Surg. 2016 Jan 6;11:4. (License: CC BY-4.0)
Bakar SM, Shamim M, Alam GM, Sarwar M. Negative correlation between age of subjects and length of the appendix in Bangladeshi males. Arch Med Sci. 2013 Feb 21;9(1):55-67.(License: CC BY-NC-ND-3.0)