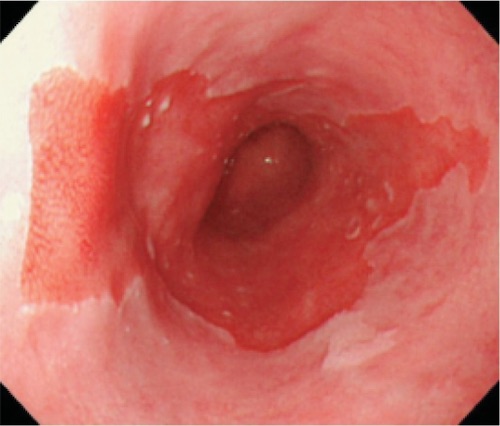
Barrett’s Esophagus 1
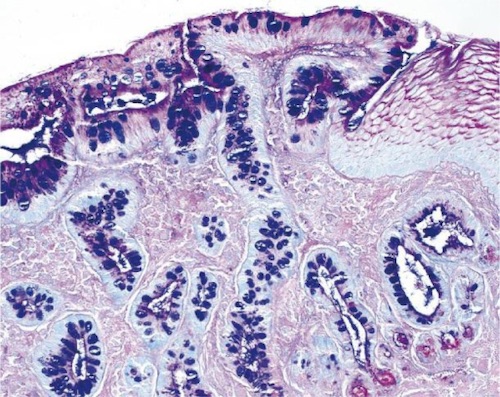
Columnar Metaplasia 2
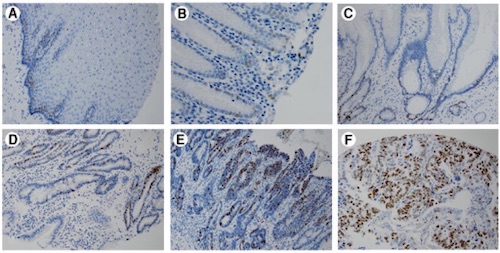
Immunohistochemical Analysis of Ki67 Expression: (A) Squamous Mucosa, (B) Columnar Metaplasia, (C) Barrett’s, (D) Low-Grade Dysplasia, (E) High-Grade Dysplasia, (F) Adenocarcinoma 3
Barrett’s Esophagus 1
Columnar Metaplasia 2
Immunohistochemical Analysis of Ki67 Expression: (A) Squamous Mucosa, (B) Columnar Metaplasia, (C) Barrett’s, (D) Low-Grade Dysplasia, (E) High-Grade Dysplasia, (F) Adenocarcinoma 3