
Complete Extrahepatic Biliary Atresia 1

Acholic Stools 2
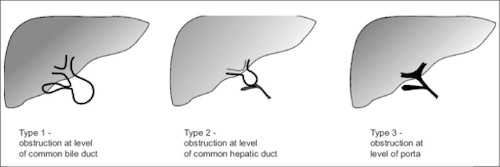
Biliary Atresia Japanese Classification 3
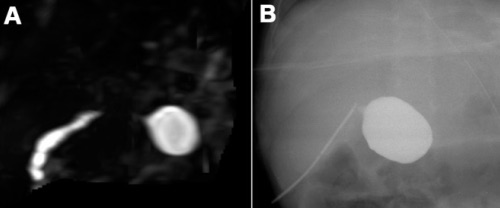
Biliary Atresia, (a) MRCP, (b) IOC 4
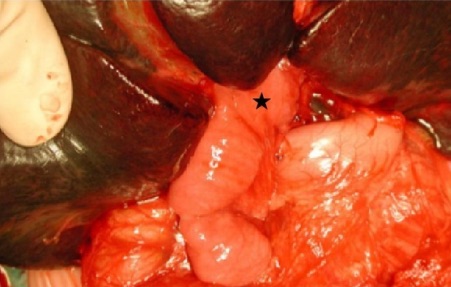
Kasai Procedure 2
Complete Extrahepatic Biliary Atresia 1
Acholic Stools 2
Biliary Atresia Japanese Classification 3
Biliary Atresia, (a) MRCP, (b) IOC 4
Kasai Procedure 2