Basics
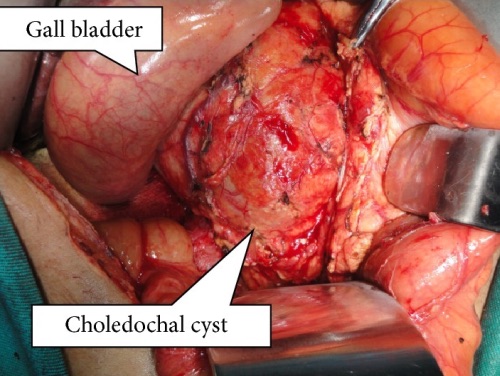
- Cystic Dilations of Intrahepatic or Extrahepatic Bile Ducts
- Previously Termed “Choledochal Cyst”
- Most Common in Females & Asians
- Risk for Malignancy
Causes
- Pancreatic Enzyme Reflux due to Anomalous Pancreaticobiliary Junction (ABPJ) During Development
- Long Common Channel Allows Free Reflux of Pancreatic Secretions into the Biliary Tract Which Causes Inflammation & Increased Pressure
- High Association
- Congenital
- Biliary Atresia
- Acquired – After Cholecystectomy or Sphincter of Oddi Dysfunction
Presentation
- Classic Triad: Abdominal Pain, Jaundice & RUQ Mass
- Sx:
- Abdominal Pain
- Cholelithiasis
- Jaundice
- Pancreatitis
- Early Satiety
- Cholangitis
- Palpable Abdominal Mass
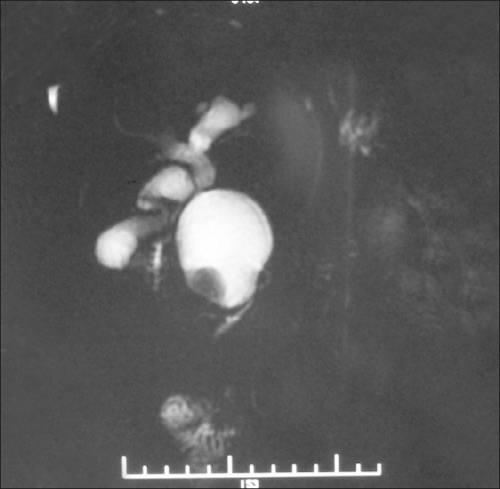
Diagnosis
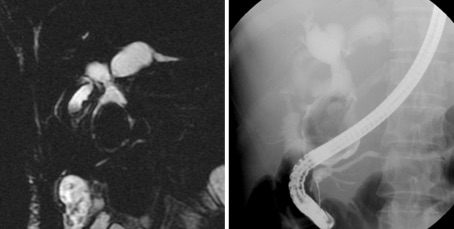
- MRCP – The Preferred Dx Test
- ERCP & Percutaneous Transhepatic Cholangiography – Most Sensitive but More Invasive
- Other Options: US or CT
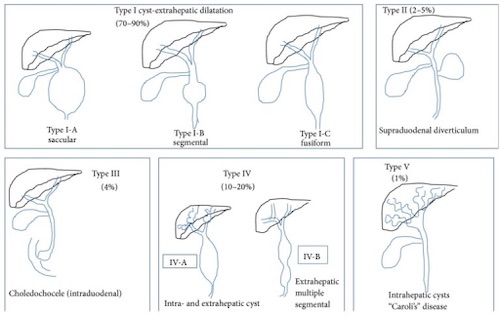
Todani Classification (See Images Below)
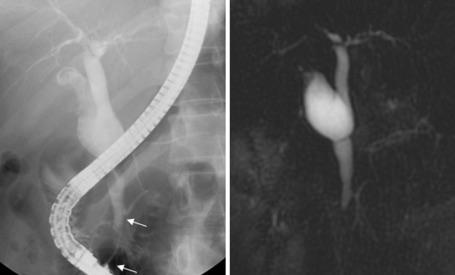
- I: Extrahepatic (Fusiform/Saccular) – Most Common
- IA – Cystic Dilation
- IB – Focal Segment (Most Common at Distal CBD)
- IC – Fusiform Dilation of Entire Extrahepatic Biliary Tract
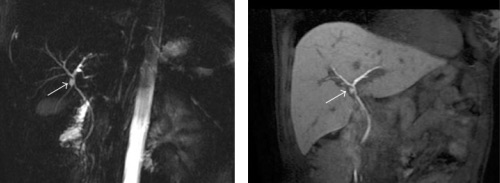
- II: Diverticula
- Not Associated with APBJ & Low Malignancy Risk
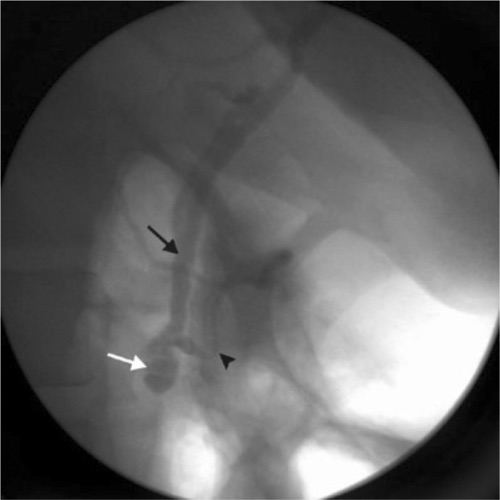
- III: Intraduodenal (Choledochocele)
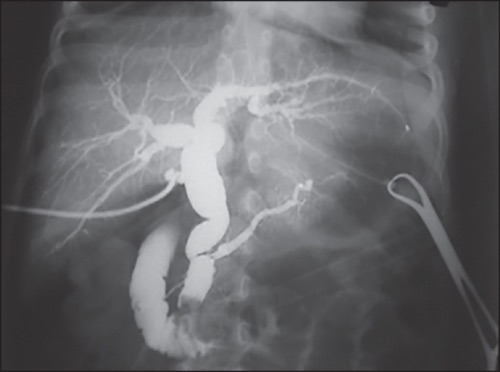
- IV: Multiple – Second Most Common
- IVA – Both Intrahepatic & Extrahepatic
- IVB – All Extrahepatic
- V: Intrahepatic (Caroli’s Disease)