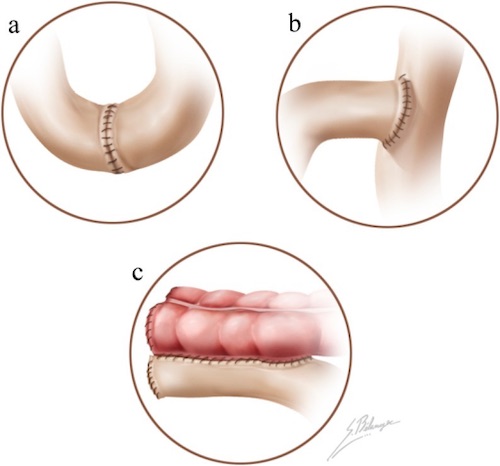
Anastomosis; (a) End-to-End, (b) End-to-Side, (c) Side-to-Side 1
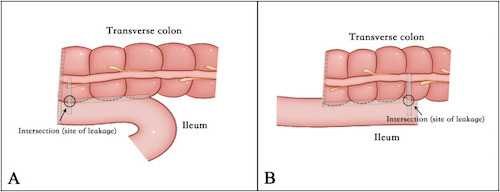
Side-to-Side Anastomosis; (A) Antiperistaltic, (B) Antiperistaltic 2
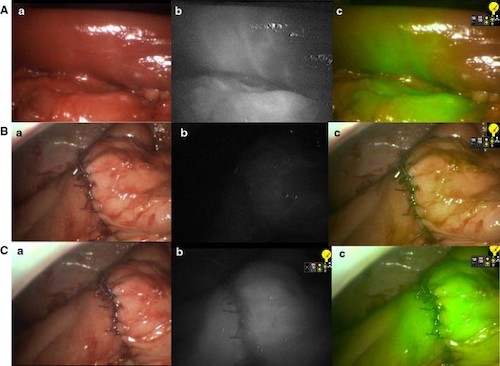
Right Hemicolectomy by ICG-FA; (A) Bowel After Vessel Division with Demarcation, (B) Anastomosis Before ICG, (C) Anastomosis After ICG; (a) Normal Light, (b) NIR, (c) Superimposition of NIR in Green 3