Urology: Benign Prostatic Hyperplasia (BPH)
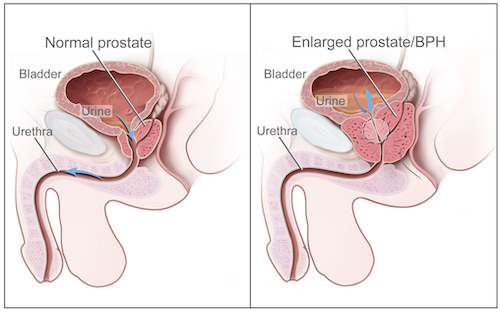
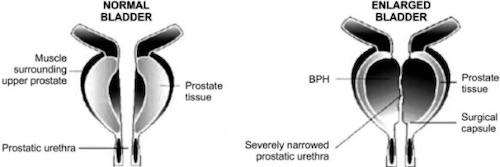
Benign Prostatic Hyperplasia (BPH)
Definitions
- Benign Prostatic Hyperplasia (BPH) – Noncancerous Increase in Prostatic Cell Number
- *Occurs in the Transitional Zone of the Prostate
- Benign Prostatic Hypertrophy – Noncancerous Increase in Prostatic Cell Size
- *Outdated Term No Longer Used
- Benign Prostatic Enlargement (BPE) – Noncancerous Overall Enlargement of the Prostate
- Benign Prostatic Obstruction (BPO) – Noncancerous Urethral Obstruction Due to Prostate Enlargement
Risk Factors
- Older Ager
- Diabetes
- Heart Disease
- Obesity
- Higher Caffeine/Coffee Intake
Lower Urinary Tract Symptoms (LUTS)
- Urinary Storage:
- Urgency – Sudden Strong Urge to Void
- Nocturia – Multiple Nighttime Voids
- Frequency
- Incontinence – Involuntary Leakage
- Urinary Voiding:
- Hesitancy – Difficulty Initiating Stream
- Weak/Slow Stream
- Intermittency – Intermittent Stream
- Straining – Difficulty in Voiding Requiring Muscular Effort
- Dysuria
- Post-Void:
- Retention/Incomplete Emptying
- Post-Void Dribble
Diagnosis
- Made by the Presence of Lower Urinary Tract Symptoms (LUTS) Without any Evidence of Other Causes
- Biopsy Unnecessary for Diagnosis (Only Required if Concern for Cancer)
BPH 1
Prostate Hyperplasia 2
Treatment
Medical Treatment
- Alpha-1-Receptor Antagonist
- Ex: Tamsulosin (Flomax), Doxazosin, or Terazosin
- First Line Medication to Relieve Symptoms
- Mechanism: Relax Smooth Muscle
- 5-Alpha-Reductase Inhibitor
- Finasteride (Proscar/Propecia)
- Mechanism: Inhibits Testosterone Conversion to Dihydrotestosterone
- Prevents Growth – May Take Months to See Effects
- Generally Used as a Combination Therapy with Alpha-1-Receptor Antagonist if Symptoms Moderate-Severe
Surgical Treatment
- Indications for Surgical Treatment:
- Failure of Medical Therapy (Urinary Retention or Moderate-Severe Symptoms)
- Recurrent UTI
- Recurrent Significant Hematuria
- Recurrent Stones
- Renal Failure Secondary to Hydronephrosis
- Surgical Procedures:
- Simple Prostatectomy
- Open, Laparoscopic or Robotic
- Generally Reserved Only for Large-Very Large Prostates
- Transurethral Resection of the Prostate (TURP)
- Most Common Procedure
- Transurethral Vaporization of the Prostate (TUVP)
- Transurethral Incision of the Prostate (TUIP)
- Photo-Selective Vaporization of the Prostate (PVP/Laser-TURP)
- Laser Enucleation of the Prostate
- Holmium Laser Enucleation of the Prostate (HoLEP)
- Thulium Laser Enucleation of the Prostate (ThuLEP)
- Robotic Waterjet Ablation of the Prostate
- Transurethral Microwave Therapy (TUMT)
- Simple Prostatectomy
Transurethral Resection of Prostate (TURP)
- Procedure: Resectoscope Inserted Through the Urethra to Resect Excess Prostatic Tissue Piecemeal & Irrigation is Used to Clear the Field
- Can Be Done Sharply or with Monopolar (M-TURP) or Bipolar (B-TURP) Electrocautery
- Complications:
- Ejaculatory Dysfunction (65-75%)
- Retrograde Ejaculation into the Bladder (Dry Orgasm)
- Due to Damage to the Nerves/Muscles Around the Bladder Neck
- Not Harmful but Decreases Fertility
- The Most Common Long-Term Complication
- UTI (1.7-8.2%)
- Erectile Dysfunction (10%)
- Urethral Stricture (2.2-9.8%)
- Bladder Neck Contracture (0.3-9.2%)
- Urinary Incontinence (30-40%)
- Bleeding
- TURP Syndrome (< 1%)
- Ejaculatory Dysfunction (65-75%)
TURP Syndrome
- Definition: Fluid Overload with Dilutional Hyponatremia Due to Water Irrigation During TURP
- Occurs 15 Minutes to 24 Hours After
- Increased Risk for Longer Procedures (> 1 Hour) or Larger Resections
- Presentation:
- Neurologic Symptoms (Headache, Confusion, Cerebral Edema, & Seizures)
- Visual Disturbance/Blindness
- Respiratory Distress
- Nausea & Vomiting
- Acute Renal Failure
- Hypertension
- Treatment: Hypertonic Saline & Diuresis (Furosemide/Lasix)
References
- National Institute of Health. Wikimedia Commons. (License: Public Domain)
- Dhingra N, Bhagwat D. Benign prostatic hyperplasia: An overview of existing treatment. Indian J Pharmacol. 2011 Feb;43(1):6-12. (License: CC BY-2.0)