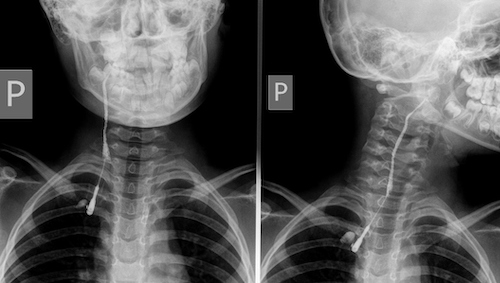
Lang S, Kansy B. Cervical lymph node diseases in children. GMS Curr Top Otorhinolaryngol Head Neck Surg. 2014 Dec 1;13:Doc08. (License: CC BY-NC-ND-3.0)
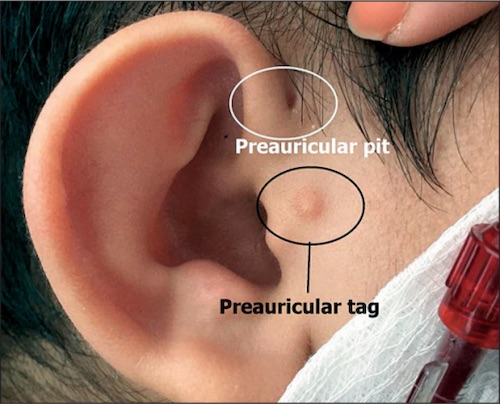
Spahiu L, Merovci B, Ismaili Jaha V, Batalli Këpuska A, Jashari H. Case report of a novel mutation of theEYA1 gene in a patient with branchio-oto-renal syndrome. Balkan J Med Genet. 2017 Mar 4;19(2):91-94. (License: CC BY-NC-ND-4.0)