Basics
- Definition: Proliferation of Ductal Cells without Basement Membrane Invasion
- The Lesion Itself Is Premalignant
- Poses an Ipsilateral Risk for Future Breast Cancer
Presentation
- Most Are Asymptomatic (No Lump or Pain) at Time of Diagnosis
- Most Often Found Incidentally
Diagnosis
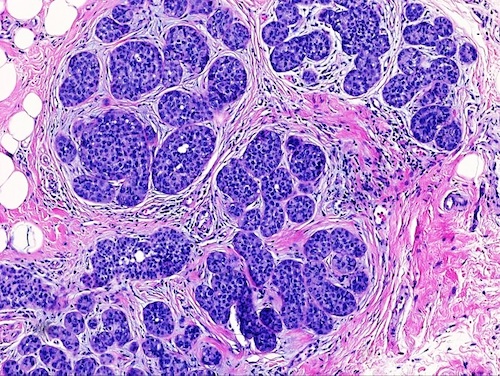
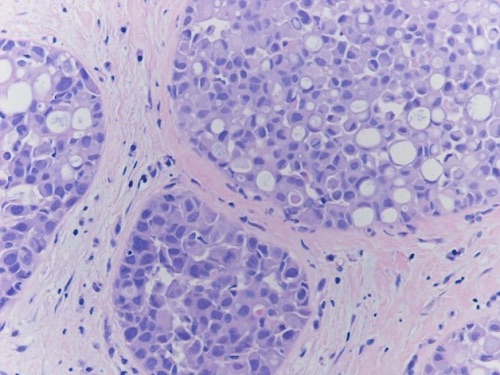
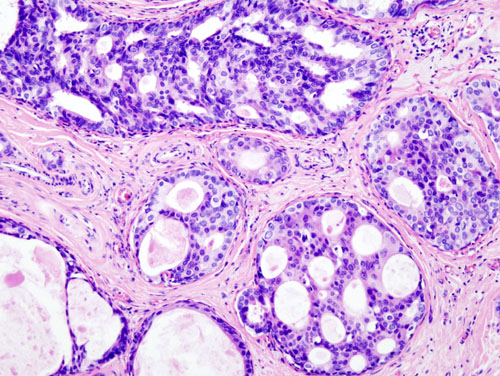
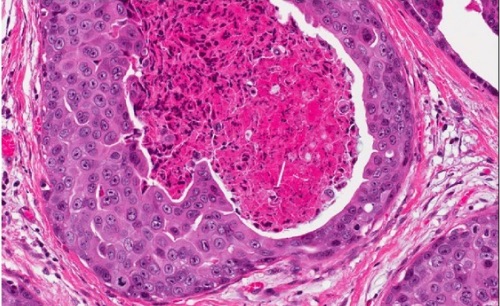
Histologic Classification
- Comedo Type: Prominent Central Necrosis (Most Aggressive Type)
- Rapid Growth Past Blood Supply
- Cribriform Type: Formation of Back-to-Back Glands without Intervening Stroma
- Micropapillary Type: Intraluminal Projections Perpendicular to the Basement Membrane without Fibrovascular Cares
- Papillary Type: Intraluminal Projections Perpendicular to the Basement Membrane with Fibrovascular Cares
- Solid Type: Tumor Cells that Distend & Fill Involved Spaces without Necrosis, Fenestrations or Papillations
- *Can Also Be Classified Based on Histologic Grade (Low, Intermediate or High)
TNM Staging
- DCIS is Designated Tis (Stage 0)
Treatment
- Primary Treatment: Surgical Lumpectomy & Adjuvant Radiation Therapy
- Margins: 2 mm
- Reasoning: Spreads Along Basement Membrane So Need Margin
- If Both DCIS & Invasive Cancer are Present, Goal is “No Ink on Tumor”
- Behaves More Like Invasive Cancer
- 10-50% Require Reoperation for Close/Positive Margin
- Consider Mastectomy for Patient Preference or if Adequate Margins Cannot Be Achieved by Lumpectomy
- Adjuvant Radiation Reduces Risk of Ipsilateral Recurrence by 50%
- No Survival Benefit
- Low-Risk Lesions May Consider Excision Alone without Radiation Therapy
- Does Not Require SLNB
- SLNB is Indicated if Preforming a Mastectomy (Unable to do SLNB in the Future)