
Breast Implant 1
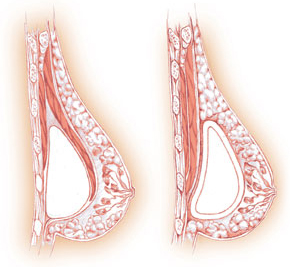
Sub-Pectoral (Left), Pre-Pectoral (Right) 2
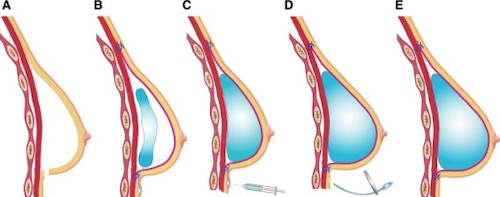
Tissue Expander Sequentially Filled 3
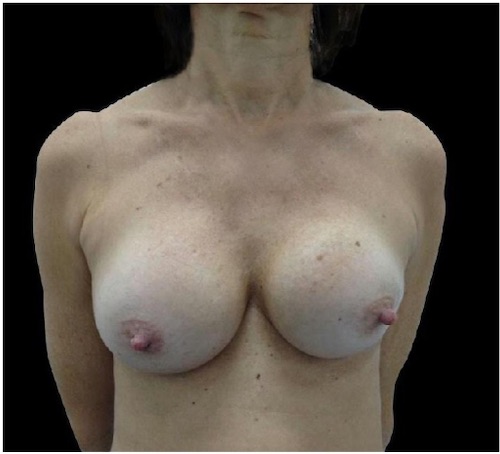
Capsular Contracture 4
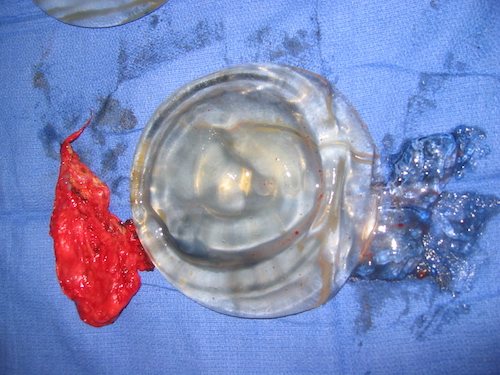
Ruptured Implant 5
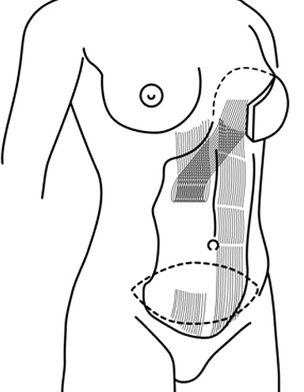
TRAM Flap 6
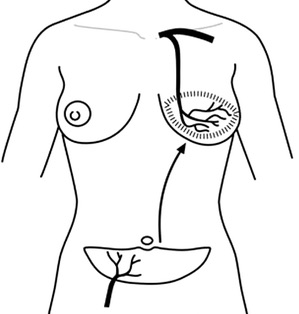
DIEP Flap 6
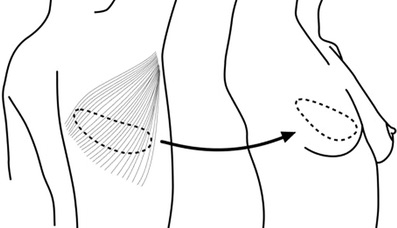
LDMF Flap 6
Breast Implant 1
Sub-Pectoral (Left), Pre-Pectoral (Right) 2
Tissue Expander Sequentially Filled 3
Capsular Contracture 4
Ruptured Implant 5
TRAM Flap 6
DIEP Flap 6
LDMF Flap 6