Carcinoid Tumor in Ileum 1

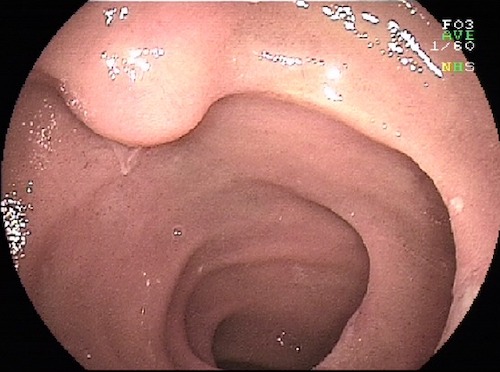
Carcinoid Tumor in Jejunum 2
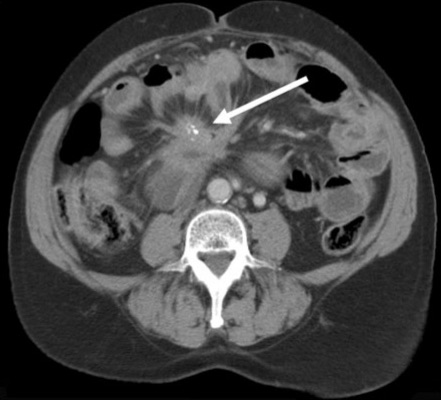
Carcinoid Tumor with Calcified Mesenteric Mass 3
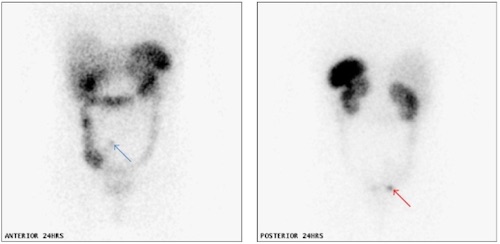
Carcinoid Tumor on Octreotide Scan 4
Carcinoid Tumor in Ileum 1
Carcinoid Tumor in Jejunum 2
Carcinoid Tumor with Calcified Mesenteric Mass 3
Carcinoid Tumor on Octreotide Scan 4