Age to Repair: 10-15 Years (Pubertal Growth Spurt – Costal Cartilage Still Compliant But Lower Risk of Recurrence)
Improves: MVP, Not Lung Volumes
Surgical Procedures
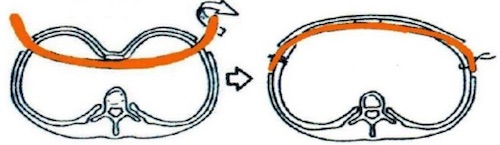
Nuss Procedure (Minimally Invasive)
Generally the Preferred Procedure
Procedure: Pass A Stainless-Steel Bar Through the Anterior Mediastinum to Stabilize
Typically Removed After a Few Years
If Metal Allergy:
Preoperatively: Use Titanium (Less Malleable & More Expensive)
Postoperatively: Steroids
If Malpositioned or Moves: Reposition & Stabilize Bar
Ravitch Procedure (Open)
Procedure:
Resect Abnormal Subperichondrial Cartilage
Sternal Osteotomy to Reposition
Internal Fixation with Retrosternal Strut
If Sternum Angled/Superior Cartilage Protruding
Pectus Excavatum 1
Nuss Procedure 2
Nuss Procedure 3
Pectus Carinatum (Pigeon Chest)
Basics
Sternum Protrudes Forward
More Common in Males
Most Often Present After Age 11
Often Worsens During Pubertal Growth Spurt
Types
Chondrogladiolar Prominence
Most Common
Middle & Lower Portions Protrude Forward
Chondromanubrial Prominence
Upper Portion Protrudes Forward
Body is Deviated Posteriorly
Lower Portion Protrudes Forward
Characteristic Z-Shape on Lateral View
Presentation
Generally Asymptomatic
May Cause Pain or Exercise Intolerance
A Large Portion Have Emotional Distress
Body Image Concerns May Cause Depression
Treatment
Primary Tx: Bracing
Indications:
Emotional Distress
Respiratory Symptoms
65-80% Success Rates
Generally Required for 4-8 Months
High Noncompliance with Therapy
If Severe or Unable to Tolerate Bracing: Open Ravitch Procedure
*See Pectus Excavatum
Pectus Carinatum 4
Pectus Carinatum Brace 5
References
Ahellwig. Wikimedia Commons. (License: CC BY-SA-3.0)
Koizumi T, Mitsukawa N, Saiga A, Satoh K. Clinical application of Nuss procedure for chest wall deformity in Poland syndrome. Kardiochir Torakochirurgia Pol. 2014 Dec;11(4):421-3. (License: CC BY-NC-ND-3.0)
Zhong W, Ye J, Liu J, Zhang C, Zhao M. Numerical Simulation and Clinical Verification of the Minimally Invasive Repair of Pectus Excavatum. Open Biomed Eng J. 2014 Dec 31;8:147-52. (License: CC BY-NC-3.0)
Jprealini. Wikimedia Commons. (License: CC BY-SA-4.0)
Jung J, Chung SH, Cho JK, Park SJ, Choi H, Lee S. Brace compression for treatment of pectus carinatum. Korean J Thorac Cardiovasc Surg. 2012 Dec;45(6):396-400. (License: CC BY-NC-3.0)