General
- Significant Force Required to Fracture, Often Multiple Injuries Present
- No Increased Concern for Underlying Cardiac Contusion
- *Previously Believed to Be
Most Common Associated Injuries
- Rib Fracture (57.8%) – Most Common
- Lung Contusion (33.7%)
- Pneumothorax (22.0%)
- Vertebral Fracture (21.6%)
- Lumbar Vertebrae Fracture (16.9%)
- Concussion (3.9%)
- Blunt Cardiac Injury (3.6%)
Diagnosis
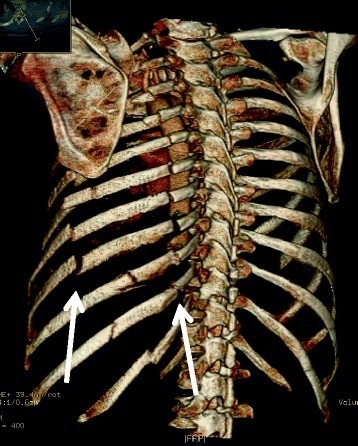
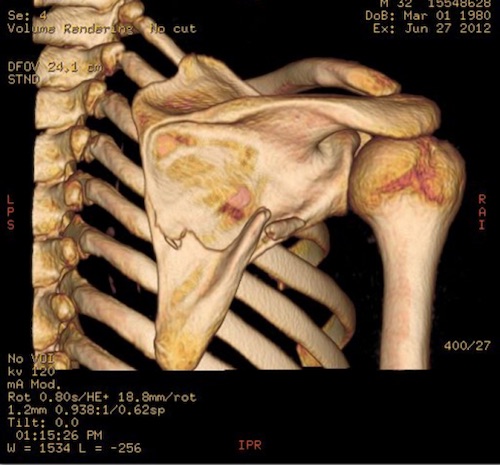
- Dx: CT
- CXR Only 50% Sensitive
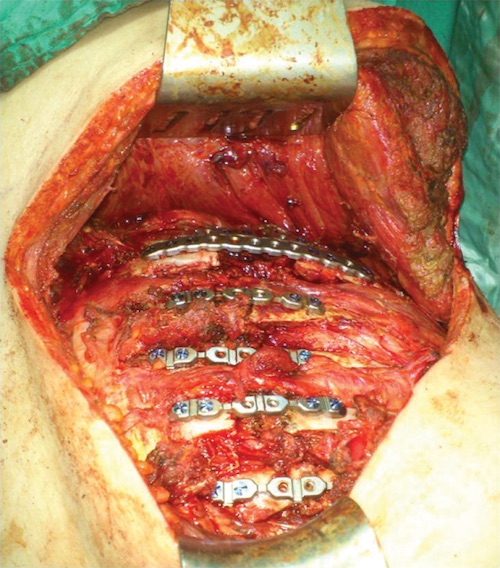
Treatment
- Tx: Supportive
- ORIF Indications: Chronic Pain or Unstable