Stronger Indication if Concomitant with a Duodenal Switch
Spinal Cord Trauma
Some Consider a Relative Indication
Symptoms Not Necessarily Obscured by Injury
Hydrops Gallbladder
Hydrops Gallbladder
Mucus Distention (Bile Absorbed, Mucus Secreted)
From Impacted Stone Without Infection
Sx: Palpable but Nontender
No Increased Risk of Malignancy
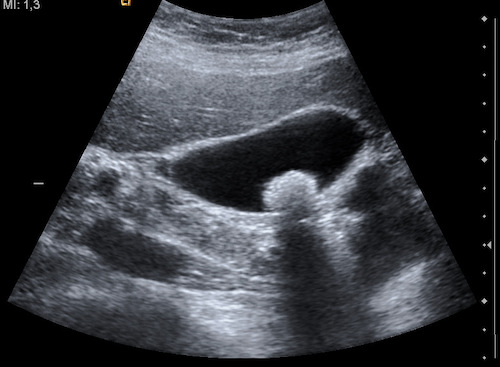
Symptomatic Cholelithiasis (Biliary Colic)
Basics
Pain from Intermittent Cystic Duct Obstruction by Gallstones
“Biliary Colic” is a Misnomer – Pain is Constant for Several Hours (Does Not Wax/Wane)
Presentation
Intense Dull RUQ Pain
Lasts 30 Minutes-6 Hours
Usually Constant, Not “Colicky”
Worse After Fatty Meal, Triggering Gallbladder Contraction
Associated with Nausea and Vomiting
Treatment
Definitive Treatment: Elective Cholecystectomy
Medical Option if Refuses Surgery: Ursodeoxycholic Acid (Rarely Used)
Dissolution Therapy
Only for Symptomatic Small Stones (< 1 cm) with a Functioning Gallbladder
40% Success but 50% Recurrence in 5 Years if Therapy Stopped
Mnemonics
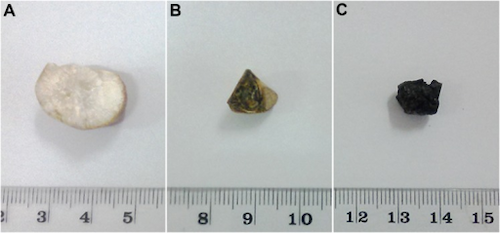
Risk Factors for Gallstones
4 F’s: “Fat Fertile Female in Her Forties”
*Some Say “5 F’s” Including “Fair” – This However is Based on the Misconception that Gallstones are Most Common in Caucasians When in Actuality they are More Common in Hispanics & Native Americans
References
Weerakoon H, Navaratne A, Ranasinghe S, Sivakanesan R, Galketiya KB, Rosairo S. Chemical characterization of gallstones: an approach to explore the aetiopathogenesis of gallstone disease in Sri Lanka. PLoS One. 2015 Apr 8;10(4):e0121537. (License: CC BY-4.0)
Nevit Dilmen. Wikimedia Commons (License: CC BY-SA-3.0)