Basics
- Majority Are < 1.0 cm (60-75%)
- Left-Sided Predominance
Size
- Small: < 5 mm
- Medium: 5-10 mm
- Large: > 1-2 cm
- Giant: > 3 cm
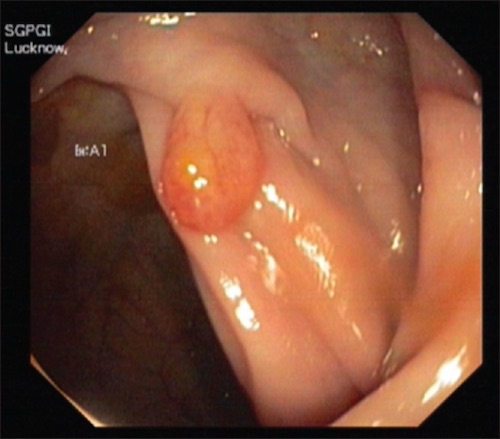
Paris Classification (Gross Appearance)
- 0-I: Polypoid
- 0-Ip: Pedunculated – Stalk at Base is Narrower than the Top
- 0-Is: Sessile – Base Has the Same Diameter as the Top
- 0-II: Nonpolypoid
- 0-IIa: Slightly Elevated
- 0-IIb: Flat – Height Less Than Half the Diameter
- 0-IIc: Depressed – Depression within the Surrounding Mucosa
- 0-III: Excavated – Ulcerated (High Risk of Malignancy)
Histologic Type
- Hyperplastic
- Normal Cellular Components with Proliferative Characteristics but No Dysplasia
- Most Common Polyp
- Characteristic Serrated (“Saw Tooth”) Pattern
- Benign
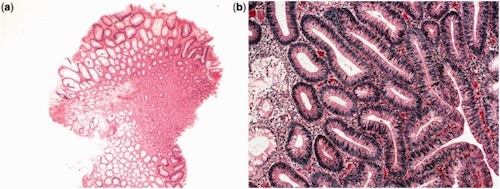
- Adenomas
- Tubular Adenoma
- > 75% Tubular Features – Network of Branching Adenomatous Epithelium
- Most Common Neoplastic Polyp
- Usually Pedunculated
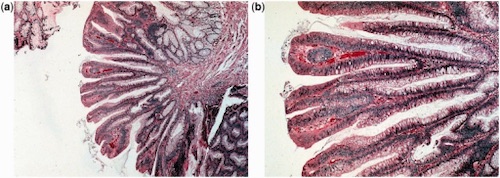
- Villous Adenoma Mn
- > 75% Villous Features – Long Glands Extending from the Surface Straight Down
- Most Likely to Produce Symptoms
- 50% Have CA
- Tubulovillous
- ≥ 25% of Both Tubular & Villous Features
- Hamartomas
- Disorganized Growth of Normal Tissue Elements
- Benign, But Can Degenerate to Adenomatous
Depth of Invasion Classification
- Haggitt Classification
- Depth of Invasion of a Malignant Pedunculated Polyp
- Levels:
- Level 0: Does Not Invade Muscularis Mucosae (In Situ)
- Level 1: Invades Head
- Level 2: Invades Neck
- Level 3: Invades Stalk
- Level 4: Invade Base or Involved in a Sessile Polyp
- All Sessile Polyps with Invasive Carcinoma are Level 4
- Risk of Lymph Node Metastasis:
- Levels 1-3: < 1%
- Level 4: 30%
- Kikuchi Classification
- Depth of Invasion of a Malignant Sessile Polyp
- Levels:
- SM1: Superficial Third
- SM2: Middle Third
- SM3: Deep Third
- Risk of Lymph Node Metastasis:
- SM1: Low Risk (2%)
- SM2-3: High Risk (22-33%)
Nodular Lymphoid Hyperplasia
- Numerous Polyps in Small & Large Intestine
- Bx: Enlarged Submucosal Lymphoid Follicles
- Benign but Associated with Immunosuppression (HIV)
Polyp Excision
- Colon: Endoscopic Polypectomy
- Rectum: Transanal Excision
- If Ulcerated – Consider Optional Resection