If Signs of Ischemia or Perforation are Present Do Not Detorse & Proceed with Surgery
Endoscopic Detorsion Outcomes:
80-95% Success Rate
40-75% Recur if Not Resected
Perform Surgery During Index Admission
Primary Anastomosis if Stable
Unstable, Peritonitis, Necrosis or Perforation: Emergent Resection
Consider Hartmann’s Procedure (Generally Preferred) vs. Primary Anastomosis
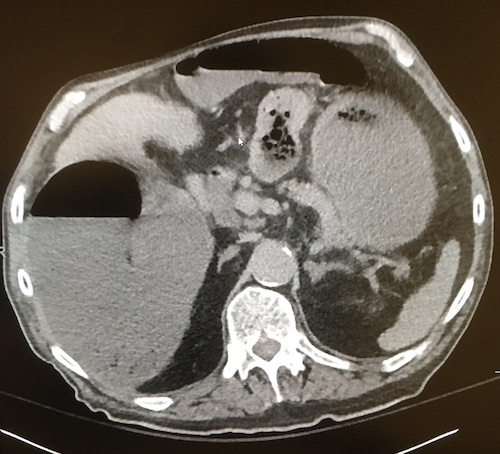
Sigmoid Volvulus 2
Sigmoid Volvulus 3
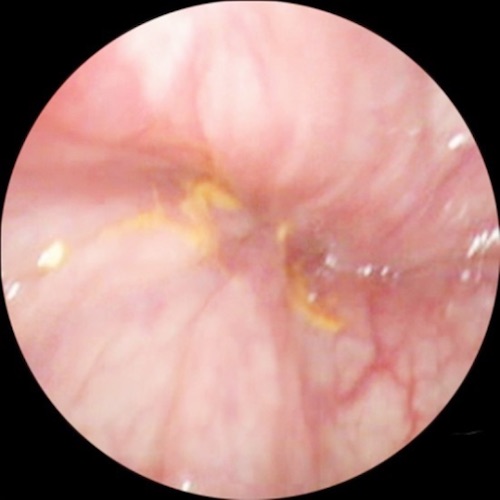
Sigmoid Volvulus Swirl on Sigmoidoscopy 4
Other Volvulus
Splenic Flexure Volvulus
More Rare Colonic Volvulus (1-2%)
Dx: Abdominal XR or CT
Tx: Surgical Resection
Avoid Endoscopic Detorsion
Transverse Colon Volvulus
More Rare Colonic Volvulus (1-4%)
Generally Younger Age
Much Higher Mortality (3x) After Resection than Cecal or Sigmoid Volvulus
Dx: Abdominal XR or CT
Tx: Surgical Resection
Avoid Endoscopic Detorsion
References
James B, Kelly B. The abdominal radiograph. Ulster Med J. 2013 Sep;82(3):179-87. (License: CC BY-NC-SA-4.0)
Elia F, Pagnozzi F, Busolli P, Aprà F. Frail patient with abdominal pain. West J Emerg Med. 2010 Sep;11(4):400-1. (License: CC BY-NC-4.0)
Qadir I, Salick MM, Barakzai A, Zafar H. Isolated adult hypoganglionosis presenting as sigmoid volvulus: a case report. J Med Case Rep. 2011 Sep 8;5:445. (License: CC BY-2.0)
Atamanalp SS, Atamanalp RS. The role of sigmoidoscopy in thediagnosis and treatment of sigmoid volvulus. Pak J Med Sci. 2016 Jan-Feb;32(1):244-8. (License: CC BY-3.0)