General
- The Most Common Digestive Complaint
Diagnostic Criteria (Rome IV) for Chronic Constipation
- ≥ 2 Of:
- Straining During ≥ 25% of Bowel Movements
- Bristol Stool Scale #1-2 ≥ 25% of Bowel Movements
- Sensation of Incomplete Evacuation ≥ 25% of Bowel Movements
- Sensation of Anorectal Obstruction ≥ 25% of Bowel Movements
- Manual Maneuvers to Facilitate ≥ 25% of Bowel Movements
- < Three Bowel Movements Per Week
- Loose Stools Rarely Present without Laxative Use
- Insufficient Criteria for Irritable Bowel Syndrome (IBS)
Causes
- Slow Colonic Transit Time
- Colonic Inertia – Delayed Transit without Defecation Abnormality
- Normal Resting Motility but Minimal Increase in After Meals
- Dyssynergic Defecation – Relaxation Failure of Puborectalis or Anal Sphincter Muscles
- Dx: Colonic Manometry or Sitz Marker Study (Swallow Radio-Opaque Markers and Follow Progression)
- Irritable Bowel Syndrome
- Diabetes
- Hypokalemia
- Hypothyroidism
- Pregnancy
- Neurologic Disorders (Multiple Sclerosis, Parkinson’s Disease or Spinal Cord Injury)
- Drugs (Opiates, Antihistamines, Iron Supplements, Antipsychotics or Antispasmodics)
Treatment
- Initial Tx: Diet & Lifestyle Modifications with Laxative Therapy
- If Medical Treatments Continually Fail: Consider Subtotal Colectomy & Ileorectal Anastomosis
- May Not Relieve Associated Symptoms Such as Abdominal Pain & Bloating – Due to High Rates of Dysmotility in Other Areas of the GI Tract
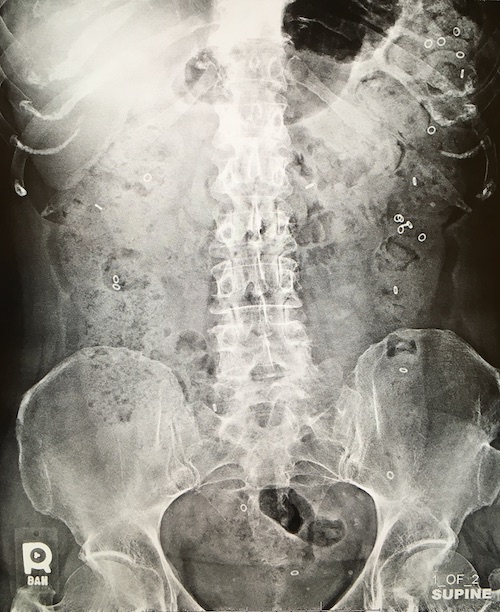
Fecal Impaction
- Massive Amount of Stool Stuck/Impacted in the Rectum or Colon
- Often from Chronic Constipation with Inability to Sense Presence of Stool in the Rectum
- Most Common in Elderly & Institutionalized Patients
- Typically in Rectum but May be More Proximal in the Sigmoid Colon
- Dx: Digital Rectal Exam (DRE) with Copious Stool in the Rectum
- Proximal Impaction May Require Abdominal XR
- Tx: Digital Disimpaction & Enema Colon Evacuation
- May Require Local Anesthesia to Relax Muscles
- Surgery if Considered for Impending Perforation or Ischemia
- Aggressive Bowel Regimen Once Disimpacted
Stercoral Ulcer
- Hard Impacted Fecaloma Causes Local Ischemia
- Caused by Chronic Constipation
- Associated with NSAID Use
- Most Common Site: Rectosigmoid Anti-Mesenteric Border
- Can Cause Pain, Bleeding or Perforation
- Usually Found Post-Perforation
- Tx: Fecal Disimpaction & Aggressive Bowel Regimen if Not Perforated