Always Vaccinate Preoperatively (Splenectomy is Commonly Performed)
Concurrent Splenectomy
Indications: High-Concern for Malignancy
Chronic Pancreatitis – Consider Preserving Although May Be Very Difficult with Inflammatory Adherence to Splenic Vein
Ligate: Splenic Artery (First), Then IMV & Finally Splenic Vein
May Preserve IMV if it is Proximal to Lesion or Enters SMV
Spleen Preserving
Indications: Benign or Cystic Mass
Ligate: Individual Branches off Splenic Artery/Vein & IMV
May Preserve IMV if it is Proximal to Lesion or Enters SMV
Complications
Pancreatic Fistula (Most Common) (30-40%)
Related More to Patient-Factors Than Operative-Technique
Risk Factors: Age ≥ 60, Obesity, Malnutrition, Absence of Epidural, Nonmalignant Pathology, Concomitant Splenectomy or Vascular Reconstruction
Not Impacted by Method of Resection, etc.
Endocrine Insufficiency – New-Onset DM
Higher Risk if Preformed for Pancreatitis
Splenic Vein Thrombosis
Bleeding
Infection/Abscess
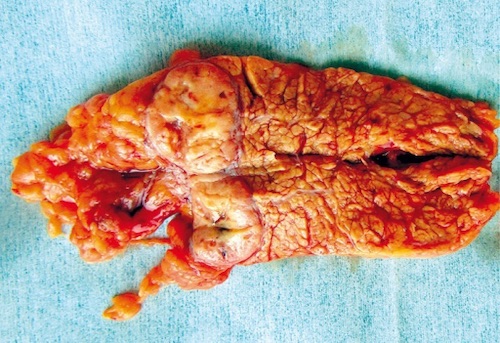
Distal Pancreatectomy 1
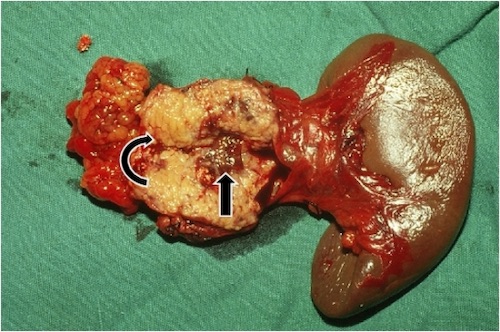
Distal Pancreatectomy with Concurrent Splenectomy 2
References
Kusnierz K, Mrowiec S, Lampe P. Results of surgical management of renal cell carcinoma metastatic to the pancreas. Contemp Oncol (Pozn). 2015;19(1):54-9. (License: CC BY-NC-ND-3.0)