If Primary Repair Not Feasible
- Under Tension or Involves Ampulla: Roux-en-Y Duodeno-Jejunostomy
- Jejunal Limb Anastomosis to the Proximal Duodenum & Oversewing of Distal Duodenum
- Massive Injury Involving Head of Pancreas: Pancreaticoduodenectomy (Whipple Procedure)
- Not Done in an Emergent Setting
- Wide Drainage at Index Operation & Definitive Repair Upon Medical Stabilization
Historical Options Fallen Out of Favor
- Jejunal Serosal Patch
- Less Desirable than Roux-en-Y
- Retrograde Jejunostomy
- For Duodenal Decompression
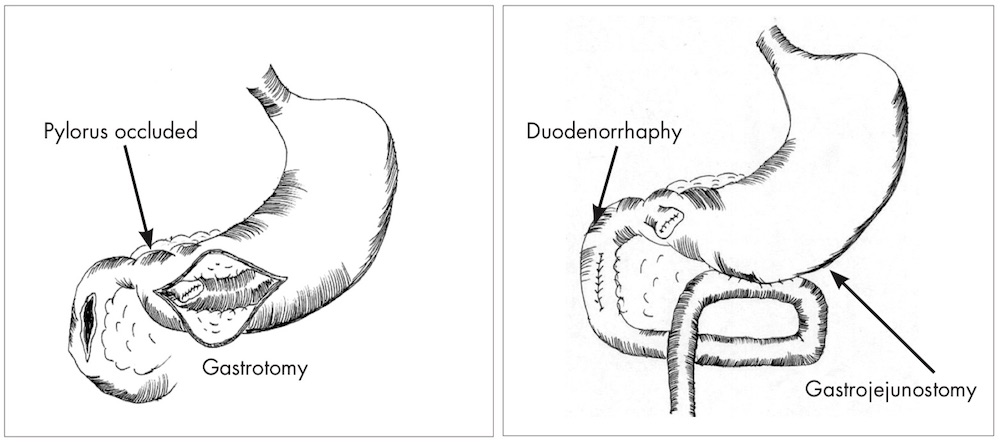
- Duodenal Diverticularization
- Procedure: Primary Repair, Antrectomy & Gastrojejunostomy
- Creates a Permanent Bypass of the Repair
- May Add Tube Duodenostomy for Decompression
- Triple-Ostomy Repair
- Procedure: Gastrostomy, Duodenostomy & Feeding Jejunostomy
- Triple-Tube Repair
- Procedure: Primary Repair with NG Tube, Feeding Jejunostomy & Retrograde Jejunostomy