Basics
- Dilation of Esophageal Veins from Portal Hypertension
- Blood Shunted Through Coronary Veins to Lower Esophagus & Azygous System
- Bleeding Risk: 5-15% Yearly
Diagnosis
- Dx: Endoscopy
- Best Non-Invasive Test: Spleno-Portal Index
- Calculated Using Doppler US
- Splenic Index (Based on Spleen Diameter)/Portal Vein Velocity
Treatment of Acute Bleeding
- Initial Tx:
- Endoscopy – Band Ligation Preferred Over Sclerotherapy (Fewer Side Effects)
- Vasoactive Medication – Telipressin (Preferred), Somatostatin or Octreotide
- Prophylactic ABX
- Rebleeds:
- First Rebleed: Second Endoscopy
- Second Rebleed: TIPS
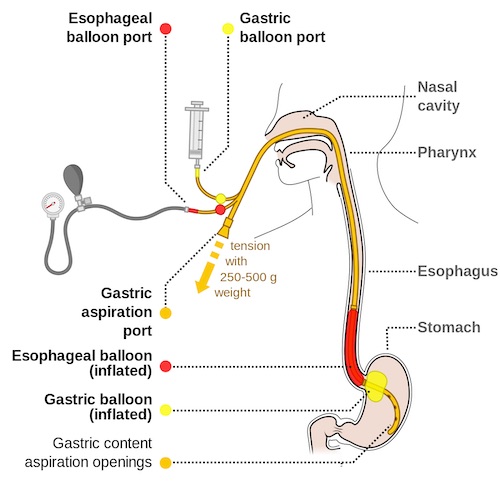
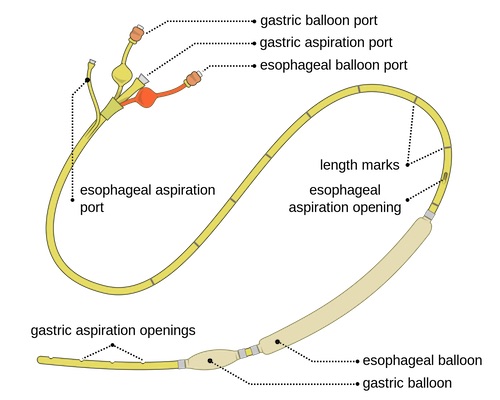
- Temporary Stabilization: Balloon Tamponade (Minnesota Tube or Sengstaken-Blakemore Tube)
- Variable Success (30-90%) but High Rebleed Risk (50%)
- Placement:
- Long Esophageal & Large Round Gastric Balloons are Inflated & Placed to Traction to Compress the GE Junction
- Distal Port Placed to Suction to Empty Luminal Contents
- Minnesota Tubes Also Have a Proximal Port to Drain Salivary Secretions – Aspiration is Most Common Complication
Cirrhosis Prophylaxis
- No Varices: Repeat Endoscopy Every 3 Years
- Small Varices: β-Blockers (Nadolol or Propranolol)
- Repeat Endoscopy Every 1-2 Years
- Medium/Large Varices: Endoscopic Ligation
- Repeat Endoscopy Every 1-2 Weeks Until Obliterated
- Then at 1-3 Months & Every 6-12 Months