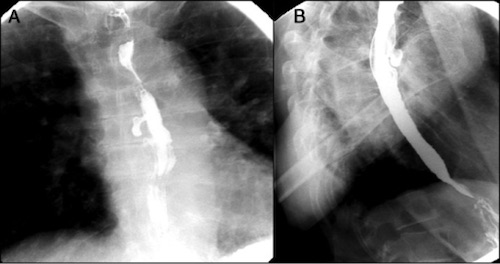
Guirguis S, Azeez S, Amer S. Sarcoidosis Causing Mid-Esophageal Traction Diverticulum. ACG Case Rep J. 2016 Dec 7;3(4):e175. (License: CC BY-NC-ND-4.0)
Silecchia G, Casella G, Recchia CL, Bianchi E, Lomartire N. Laparoscopic transhiatal treatment of large epiphrenic esophageal diverticulum. JSLS. 2008 Jan-Mar;12(1):104-8. (License: CC BY-NC-ND-3.0)