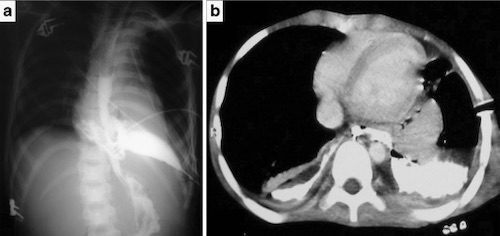
Trauma: Esophagus Trauma Esophagus GeneralMost Common in Penetrating TraumaMost Common Site: Cervical #1, Thoracic #2 & Abdominal #3Virtually All Have Other Concomitant InjuriesAAST Esophagus Injury Scale*See AASTInjury Scale is Under CopyrightDiagnosisDelay in Diagnosis CommonDx: Water-Soluble EsophagramIf Negative but High-Suspicion: Dilute-Barium EsophagramIf Again Negative: EsophagoscopySpecificity:Contrast Studies Have High False-Negative Rates (25%)Negative Esophagram & Esophagoscopy Near 100% Specificity Traumatic Esophagus Perforation with Contrast Extravasation 1 TreatmentPrimary Tx: Surgical Repair, Buttress & Leave DrainRepairFirst Extend Myotomy – To See Full Length of Mucosal InjuryClose in Two Layers: Inner Absorbable, Outer PermanentStrength Layer: Submucosa (No Serosa)Direction:Small: TransverselyLarger (> 2-3 cm): LongitudinallyIf Penetrating Injury: Explore Circumference to Verify No Back-Wall InjuryButtressStrengthens & Enhance Healing Given no Serosal LayerNeck: Strap Muscles or SCMProximal Thorax: Intercostals or Rhomboid MuscleMuscle Flaps Preferred (Less Friable & More Bulky Coverage)Other Less Desirable Options: Pericardium or PleuraDistal Thorax or Abdomen: Stomach (Nissen Fundoplication)If Unable to Perform Nissen: DiaphragmDrainsNeck: Penrose or JP DrainThoracic: Chest TubesAbdomen: JP DrainDevastating Injury (Repair Not Feasible):Neck: Cervical Esophagostomy (Spit Fistula)Loop Esophagostomy If Able – Allows One-Stage ClosureEnd Esophagostomy Requires Complex ClosureThoracic: T-Tube (Creates a Controlled Fistula) References Oikonomou A, Prassopoulos P. CT imaging of blunt chest trauma. Insights Imaging. 2011 Jun;2(3):281-295. (License: CC BY-4.0)