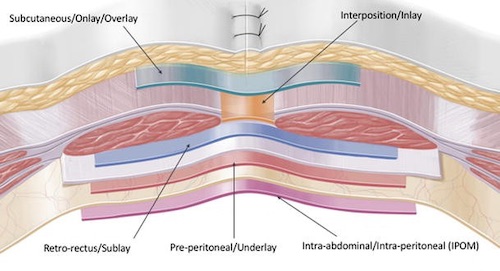
Inlay (Interposition) – Within Rectus Muscle Defects
Higher Recurrence Rate
Sublay (Retro-Rectus) – Between Rectus Muscle & Posterior Rectus Sheath
“Rives-Stoppa-Wantz” Repair
Lowest Recurrence Rate
Underlay (Preperitoneal) – Behind Posterior Rectus Sheath, Before Peritoneum
Intraperitoneal Onlay Mesh (IPOM) – In Abdominal Compartment
Mesh Considerations
Ventral Hernia Overlap Goal: Minimum of 3-5 cm
Use Permanent or Long-Acting Sutures for Securement
Permanent Mesh is More Susceptible to Infection
Better to Use Absorbable in Contaminated Field
If Inadvertent Enterotomy is Made (Without Gross Spillage) Synthetic Mesh Can Still Be Used
Routine Drain Placement Has Increased Risk of Infection
Prophylactic Mesh Placement
Decreases Risk of Recurrence
Onlay Appears to Be Superior
Complications:
Increased Risk of Seroma
No Increased Risk of Infection
*Use is Debated and Not Clearly Defined
Mesh Placement Techniques 1
References
Parker SG, Wood CPJ, Sanders DL, Windsor ACJ. Nomenclature in Abdominal Wall Hernias: Is It Time for Consensus? World J Surg. 2017 Oct;41(10):2488-2491. (License: CC BY-4.0)