
WVAC Closure 1

“Shoelace” Closure 2

Forearm Fasciotomy Incision 3
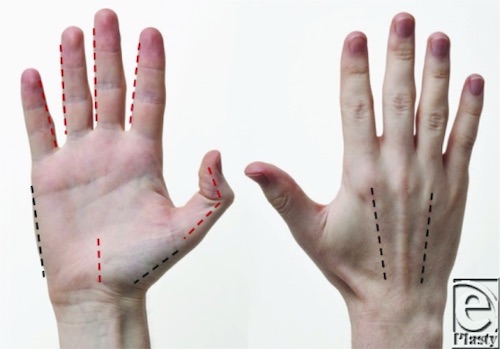
Hand Fasciotomy Incisions 4
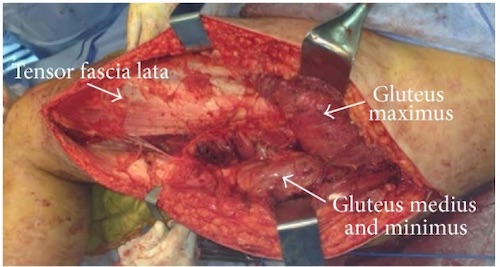
Buttock Fasciotomy 5

Thigh Fasciotomy 6

Foot Fasciotomy Incisions 7
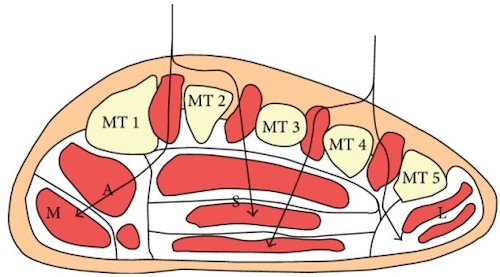
Foot Fasciotomy Depth 3
WVAC Closure 1
“Shoelace” Closure 2
Forearm Fasciotomy Incision 3
Hand Fasciotomy Incisions 4
Buttock Fasciotomy 5
Thigh Fasciotomy 6
Foot Fasciotomy Incisions 7
Foot Fasciotomy Depth 3