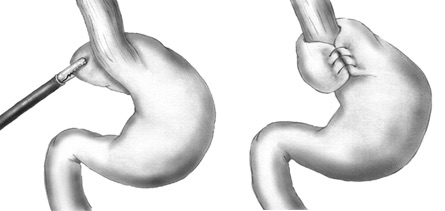
Nissen Fundoplication 1
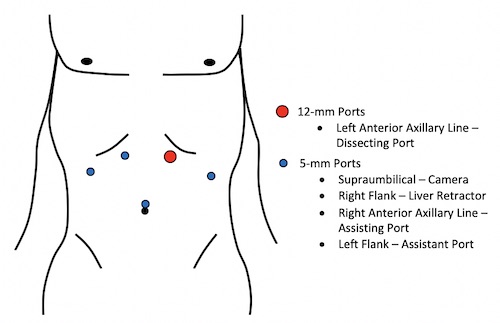
Nissen Port Placement
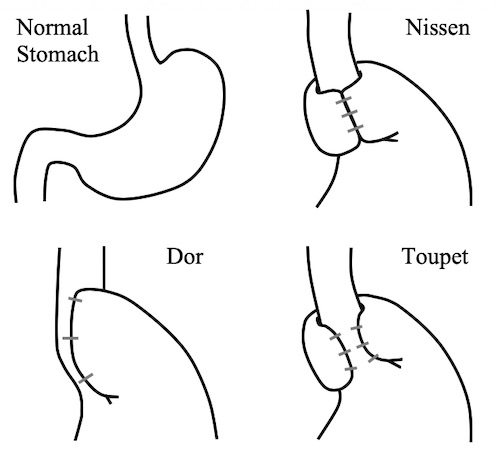
Fundoplication Types
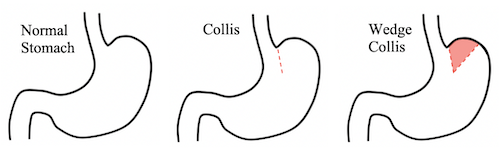
Collis Gastroplasty
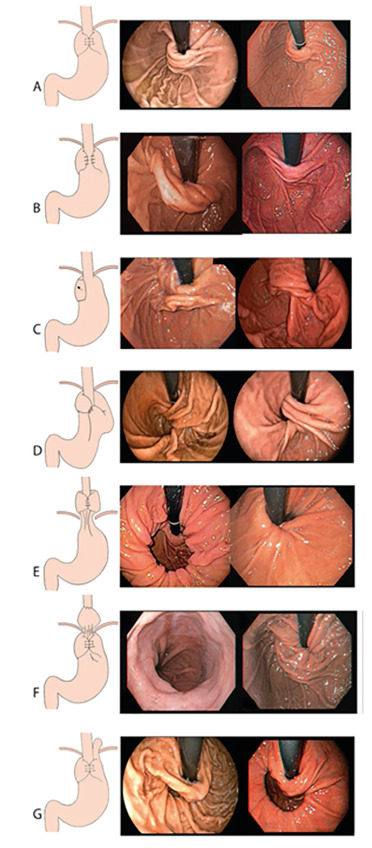
EGD Findings After Fundoplication: A) Normal Nissen, B) Partial Fundoplication, C) Disrupted Fundoplication, D) Twisted Fundoplication, E) Migrated Fundoplication, F) Slipped Fundoplication, G) Paraesophageal Hernia 2