Gastrectomy – Roux-en-Y Lower Risk Than Billroth Reconstructions
Highest Risk: Billroth II
Gastric Bypass
Esophagectomy
Vagotomy or Pyloroplasty
Ulcers
Diagnosis
Dx: Gastric Emptying Study
Treatment
Primary Tx: Dietary Changes
Frequent Small Meals
High in Fiber & Protein
Low in Carbs & Sugar
If Refractory or Severe: Octreotide (The Most Effective Treatment)
If Fails with Prior Distal Gastrectomy: Surgical Conversion to Roux-en-Y Reconstruction
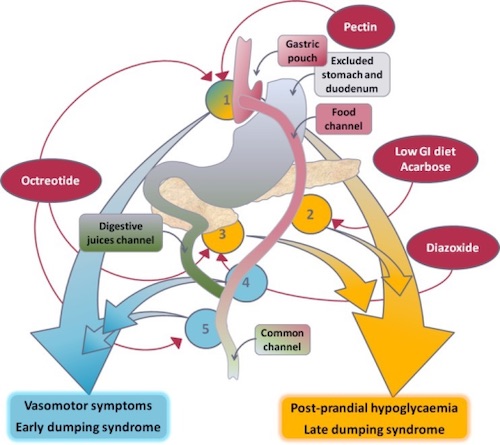
Pathophysiology of Dumping Syndrome 3
References
Vasavid P, Chaiwatanarat T, Pusuwan P, Sritara C, Roysri K, Namwongprom S, Kuanrakcharoen P, Premprabha T, Chunlertrith K, Thongsawat S, Sirinthornpunya S, Ovartlarnporn B, Kachintorn U, Leelakusolvong S, Kositchaiwat C, Chakkaphak S, Gonlachanvit S. Normal Solid Gastric Emptying Values Measured by Scintigraphy Using Asian-style Meal:A Multicenter Study in Healthy Volunteers. J Neurogastroenterol Motil. 2014 Jul 31;20(3):371-8. (License: CC BY-NC-3.0)
Shin YK, Kwon JG, Kim KY, Park JB, Han SJ, Cheon JW, Kim EY, Kim HG, Lee TS, Park KS, Won KS. A case of cyclic vomiting syndrome responding to gonadotropin-releasing hormone analogue. J Neurogastroenterol Motil. 2010 Jan;16(1):77-82. (License: CC BY-NC-3.0)
Narayanan RP, Syed AA. Pregnancy Following Bariatric Surgery-Medical Complications and Management. Obes Surg. 2016 Oct;26(10):2523-9. (License: CC BY-4.0)