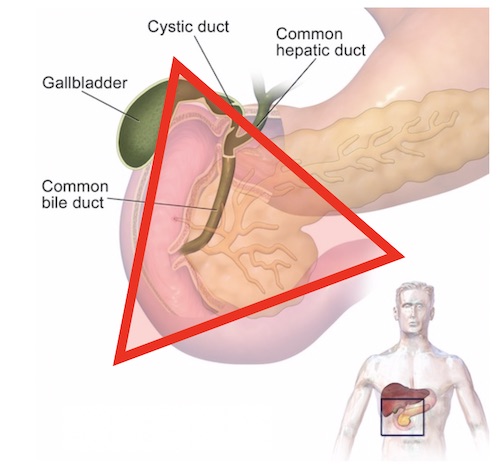
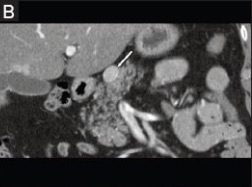
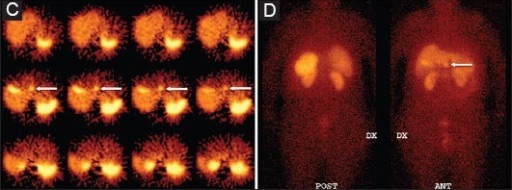
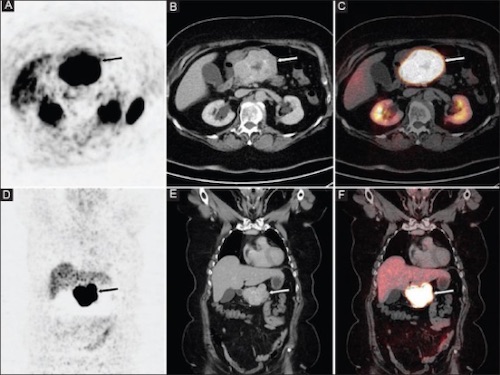
Stomach: Gastrinoma (Zollinger-Ellison Syndrome) Gastrinoma (Zollinger-Ellison Syndrome/ZES) BasicsGastrin Secreting TumorAbout Half Are Malignant (50-60%)Gastrinoma (Passaro) Triangle – Contain 80% of TumorsJunction of the Cystic & Common Bile DuctsJunction of the Second & Third Portions of the DuodenumJunction of the Neck & Body of the PancreasMost Common in MalesPresentationSevere/Refractory Peptic UlcersMost Common Ulcer Location: Proximal Duodenum (Some in Distal & Jejunum)Symptoms:PainDiarrheaGERDNausea & Vomiting Gastrinoma Triangle 1 DiagnosisScreening Tests (Non-Diagnostic):Elevated Fasting Gastrin While Off PPI for 3-7 DaysAcid Present in Gastric pH AnalysisDiagnosis: Marked Gastrin Increase After Secretin Stimulation TestWould Normally Show Minimal ChangeMust Hold PPI Prior to TestIf Unsafe to Hold PPI (Life-Threatening Bleeding, etc.): Consider Somatostatin Receptor Imaging for Diagnosis & LocalizationLocalization:Initial: CT or MRIIf Fails: Somatostatin Receptor ImagingSomatostatin (Octreotide) Receptor Scintigraphy (SRS)Classically UsedMost Sensitive TestFunctional PET ScansBecoming More Prevalent with Higher SensitivityRadiotracer: Ga-68 DOTATATE or Ga-68 DOTATOCIf Imaging Fails: EUSIf EUS Fails: Selective Arterial Stimulation with Hepatic Venous SamplingIf High Suspicion but Still Unable to Localize: Surgical ExplorationTreatmentResectable:< 2-3 cm: Enucleate> 2-3 cm, Local Invasion or N/M+: ResectionPancreatic Head/Neck: PancreaticoduodenectomyPancreatic Body/Tail: Distal PancreatectomyIf Malignancy Suspected: Concurrent SplenectomyEntire Pancreas: Total PancreatectomyUnresectable or Mets:Resect Mets if AbleSymptomatic Tx: PPIIf Fails: OctreotideIf Severe/Enlarging: ChemotherapyClassic Regimen: Streptozocin with/without Doxorubicin (Toxic to Beta Cells)Newer Regimen: Temozolomide with/without Capecitabine (CAPTEM) PNET on CT 2 PNET on EUS 2 PNET on SRS 2 PNET on Functional PET 2 References Blaus B. Wikimedia Commons (License: CC BY-SA-4.0) – AlteredKartalis N, Mucelli RM, Sundin A. Recent developments in imaging of pancreatic neuroendocrine tumors. Ann Gastroenterol. 2015 Apr-Jun;28(2):193-202. (License: CC BY-NC-SA-3.0)