Stomach: Gastrostomy
Surgical Gastrostomy
Laparoscopic Gastrostomy
- Gastrostomy Placed Under Laparoscopic Guidance
- Preformed Similar to Radiological Gastrostomy
- Procedure:
- Stomach is Anchored to the Wall with 3-4 T-Fasteners
- Needle is Inserted at the Center of the T-Fasteners to Access the Stomach
- A Guidewire is Passed through the Needle & the Needle is Removed
- A Dilator is Passed over the Guidewire & Then Removed
- The G-Tube is Then Passed Over the Guidewire & Wire is Removed
- Finally the G-Tube is Secured with an External Bolster
Stamm Gastrostomy
- Most Common Open Gastrostomy Procedure
- Typically Used as a Temporary Procedure
- Procedure:
- Place a Purse-String Suture in the Mid Anterior Wall of the Stomach
- Make an Incision in the Middle of the Purse String Along the Longitudinal Axis
- G-Tube is Then Inserted into the Stomach 10-15 cm
- First Purse-String is Secured
- A Second Purse-String is Used to Invaginate the First Purse-String
- A Separate Incision in Made Through the Abdominal Wall About 3 cm Below Costal Margin & 3 cm Left of Midline and The Tube is Brought Out
- The Stomach is Then Gastropexied to the Abdominal Wall Around the Tube
- Finally the G-Tube is Secured to the Skin
Witzel Gastrostomy
- Procedure:
- Place a Single Purse-String Suture in the Mid Anterior Wall of the Stomach
- Make an Incision in the Middle of the Purse String Along the Longitudinal Axis
- G-Tube is Then Inserted into the Stomach
- Tube is Then Laid Against the Stomach
- Additional Sutures are Placed to Imbricate the Gastric Wall Over the Tube
- The G-Tube is Then Brought Through the Skin
- Stomach is Gastropexied to the Abdominal Wall
- Finally the G-Tube is Secured to the Skin
Janeway Gastrostomy
- Mucosa Lined Permanent Procedure
- Procedure:
- A 5-6 cm Rectangular Flap is Made with Its Base Along the Greater Curvature
- Edges of the Rectangular Flap are Approximated to Form a Tube
- A G-Tube is Inserted Through the Approximated Flap
- The G-Tube is Then Brought Out Through the Abdominal Wall
- The Anterior Gastric Wall is Gastropexied to the Abdominal Wall
Percutaneous Endoscopic Gastrostomy (PEG)
General Considerations
- Gastrostomy Tube Is Placed Through the Skin with Endoscopic Guidance/Assistance
- Requires Both a Surgeon & Endoscopist
- Compared to Surgical Gastrostomy Tube: Similar Morbidity & Mortality
Contraindications
- Absolute Contraindications:
- Massive Ascites
- Unable to Pass Endoscope into Stomach
- Interposed Organs (Liver or Colon)
- Hemodynamic Instability
- Sepsis
- Uncorrectable Coagulopathy
- Abdominal Wall Infection at Access Site
- Past Total Gastrectomy
- If Being Used for Feeding: Severe Gastroparesis or Gastric Outlet Obstruction
- Relative Contraindications:
- Esophageal Cancer (Compromise Future Gastric Conduit)
- Hepatosplenomegaly
- Peritoneal Dialysis
- Portal Hypertension with Gastric Varices
- Past Partial Gastrectomy
Classic “Pull Technique” (Ponsky)
- Start with Endoscopy into Stomach to Ensure no Anatomic Obstacles & Insufflate
- Gain Access Through Abdominal Wall
- Choose Site on Abdominal Wall by Transillumination from Endoscope, Should Be About 2 cm Below Costal Margin
- Confirm Site by Endoscopically Visualizing Gastric Wall Indentation While Finger Presses on Site
- A Needle with Saline Syringe Under Negative Pressure is Inserted Through the Abdominal Wall into the Gastric Lumen
- Stool or Air Bubbles Before Entering the Stomach Indicated Bowel Passage
- OK to Retry if See Air Bubbles First
- Pull Looped Wire Through the Mouth
- Snare is Placed Around the Needle
- Soft Looped Wire is Inserted Through the Needle & Then Grabbed with the Snare
- Endoscope is Removed, Pulling the Wire through the Mouth
- The Distal End Will Still Protrude from the Abdominal Wall
- Pull PEG Tube Through the Abdominal Wall
- Wire Loop is then Secured to the PEG Tube
- The Wire is Then Pulled Back Through the Abdominal Wall, Pulling the PEG Tube with It
- Needle is Removed Once the Tube Hits the Gastric Wall
- PEG Tube is then Pulled Through the Abdominal Wall Until the Internal Bolster Rests Along the Gastric Wall
- Endoscope Reinserted to Confirm Position
- Place the External Bolster and Cut the Tube to Size
- Bolster Should Lie 1-2 cm from the Skin
- Snug but Not Too Tight (Will Necrose Stomach Wall)
“Push Technique” (Sachs-Vine)
- Initial Access Similar to “Pull Technique”
- Pull a Guidewire Through the Mouth Instead of a Looped Wire
- PEG Tube is Then Pushed Down Through the Mouth Over the Guidewire
- Once Seen Emerging the Tube is Then Pulled Through the Abdominal Wall
“Introducer Technique” (Russel)
- Endoscope Only to Insufflate & Observe
- Initial Access Similar to “Pull Technique”
- Guidewire Placed Through Needle & Needle Removed
- Introducer with Outer Sheath Passed Over Guidewire Then Sheath and Introducer Removed
- PEG Tube (Balloon Deflated) Passed Through Sheath
- Sheath Then Pulled Away
- Balloon Inflated & PEG Tube Appropriately Secured
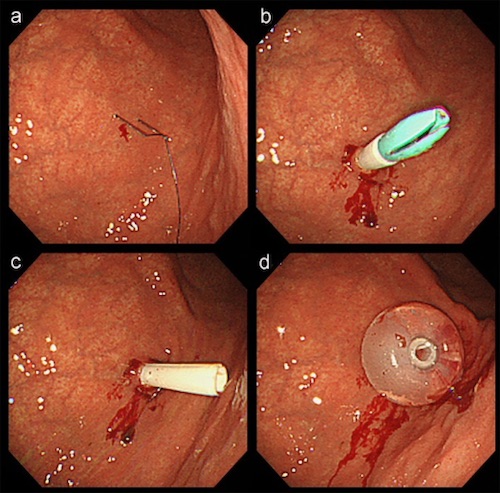
PEG (Introducer Technique) 1
Complications
- Infection
- Most Common Complication
- Give Prophylactic ABX
- Dislodged Tube
- Most Common Cause: Excessive Traction in Combative or Confused Patients
- Initial Tx: Replace at Bedside
- XR with Water-Soluble Contrast Through Tube to Confirm if < 2-4 Weeks or Any Concern for Intraperitoneal Placement
- If Fails: OR Replacement (Emergent if < 2 Weeks)
- *Some Advise Against Bedside Replacement if < 2-4 Weeks Old & Advise Letting the Tract Heal with New G-Tube Placement in a Few Days
- Peristomal Leakage
- More Likely with DM or Malnutrition with Poor Wound Healing
- If Tract is Mature (> 4 Weeks) Can Remove Tube for 24-48 Hours to Allow Tract to Close Slightly
- Tube Obstruction
- Often Clogged with Tube Feeds or Medications
- Prevention:
- All Medications Should be Either Liquid Form of Dissolved in Liquid
- Always Flush with ≥ 20-30 cc Saline/Water After Feeds or Medications
- Never Use Bulking Agents Through the Tube
- Tx: Flush with 60 cc Saline/Warm Water
- Other Options: Pancreatic Enzymes, Specialized Gastrostomy Brush or Endoscopic Cytology Brush
- Gastrocolocutaneous Fistula
- During Initial Placement PEG Penetrates Through Interposed Colon Between Abdominal Wall & Stomach
- Most Often Recognized After Removal & Replacement of the Original Tube
- Presentation:
- Sudden Onset Diarrhea – From Tube Feeds Entering Transverse Colon
- Feculent Material in PEG Tube
- Feculent Vomiting – From Retrograde Passage into Stomach
- Diagnosis: UGI
- Treatment: Removal of Feeding Tube to Allow Tract Healing
- Laparotomy if Peritonitis or Signs of Leak
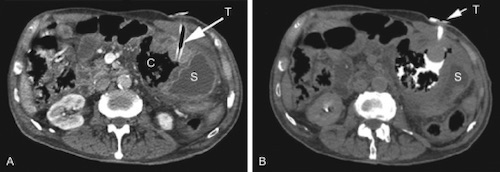
PEG Dislodged; Contrast Extravasation 2
Radiological Gastrostomy
Radiological Gastrostomy
- Gastrostomy Tube is Placed Using Fluoroscopic Guidance in IR
- Procedure:
- First Insufflate Stomach Per a Nasogastric Tube
- Stomach is Anchored to Wall with 3-4 T-Fasteners
- Needle is Inserted at the Center of the T-Fasteners to Access the Stomach
- A Guidewire is Passed through the Needle & the Needle is Removed
- A Dilator is Passed over the Guidewire & Then Removed
- The G-Tube is Then Passed Over the Guidewire & Wire is Removed
- Finally the G-Tube is Secured with an External Bolster
References
- Toh Yoon EW, Kobayashi M. Percutaneous Endoscopic Gastrostomy in a Patient With Continuous Intrathecal Baclofen Infusion Therapy. Gastroenterology Res. 2017 Apr;10(2):132-134. (License: CC BY-NC-4.0)
- Soares da Silva MQ, Lederman A, Coelho da Rocha RF, Lourenção RM. Feeding tube replacement: not always that simple! Autops Case Rep. 2015 Mar 30;5(1):49-52. (License: CC BY-NC-3.0)