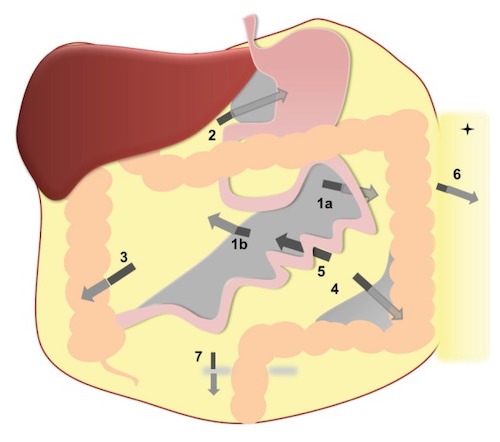
Sites of Internal Hernia: Left Paraduodenal Hernia (1a); Right Paraduodenal Hernia (1b); Foramen of Winslow Hernia (2); Pericecal Hernia (3); Sigmoid-Related Hernia (4); Transmesenteric Hernia (5); Transomental Hernia (6); Supravesical Hernia (7) 1
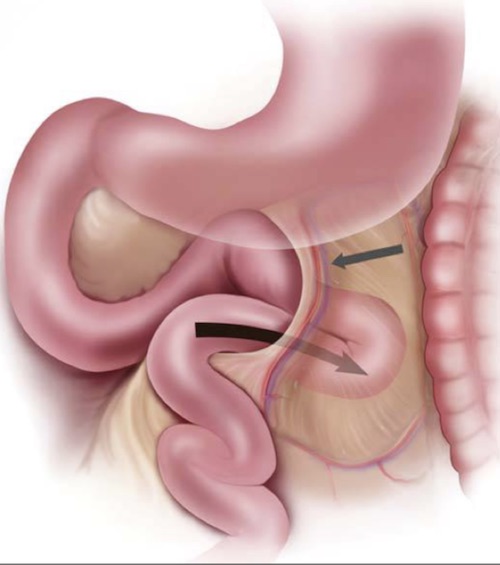
Left Paraduodenal Hernia 2
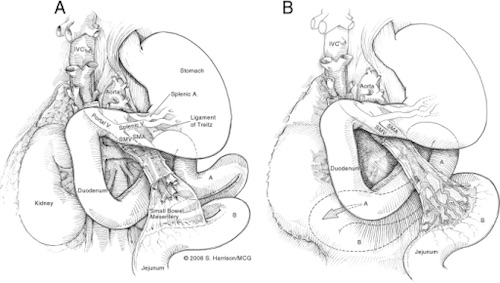
Right Paraduodenal Hernia; (A) Normal Anatomy, (B) Right Paraduodenal Hernia 3
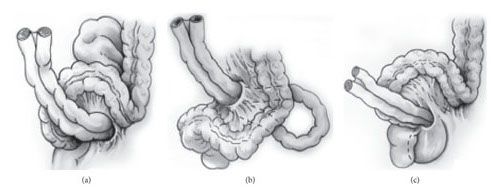
Sigmoid-Related Hernias; (a) Intersigmoid, (b) Trans-Mesosigmoid, (c) Intra-Mesosigmoid 4
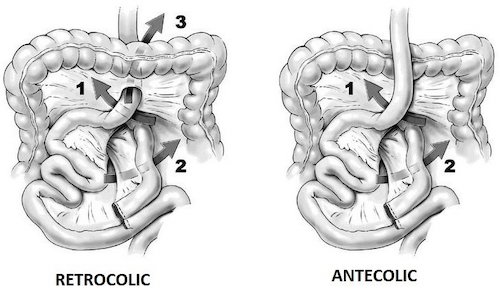
Mesenteric Defects After Roux-en-Y Gastric Bypass; (1) Petersen’s Space, (2) Brolin’s Space, (3) Transverse Mesocolic Window (Only in Retrocolic Bypass) 5
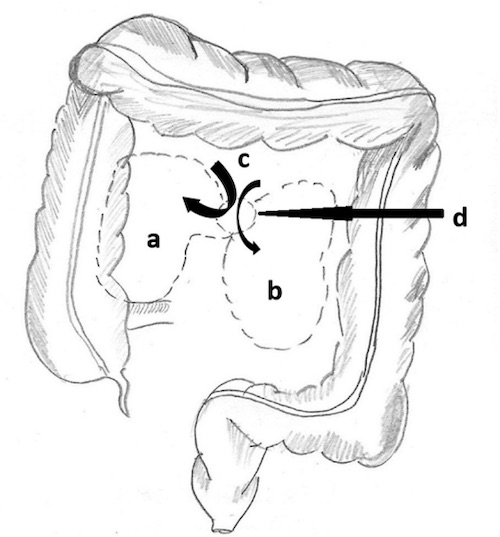
Paraduodenal Hernia Fossae; (a) Waldeyer’s Fossa, (b) Landzert’s Fossa, (c) Retroperitoneum, (d) Hernial Orifice 6
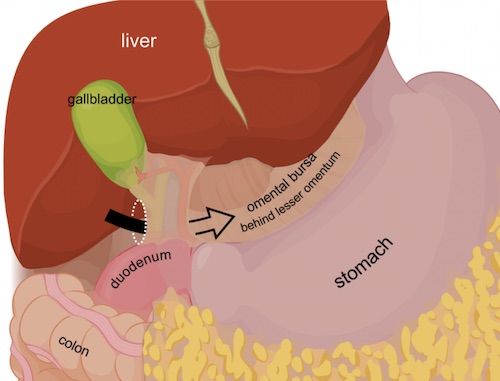
Foramen of Winslow 7
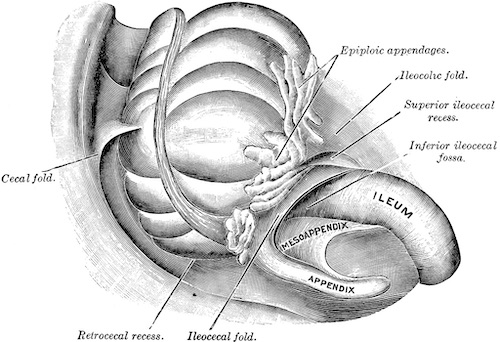
Pericecal Fossa 8
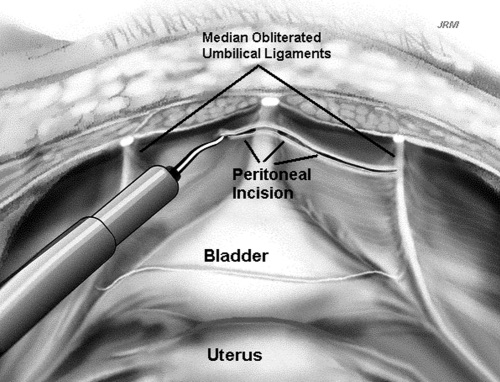
Incision into the Space of Retzius 9
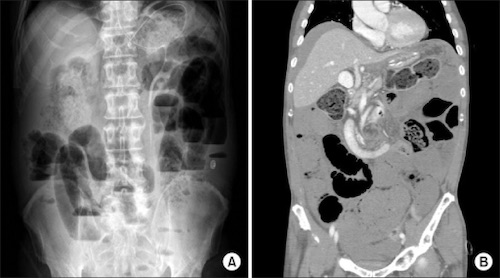
Peterson’s Hernia; (A) AXR Showing SBO, (B) CT Showing Mesenteric Swirl Sign 10