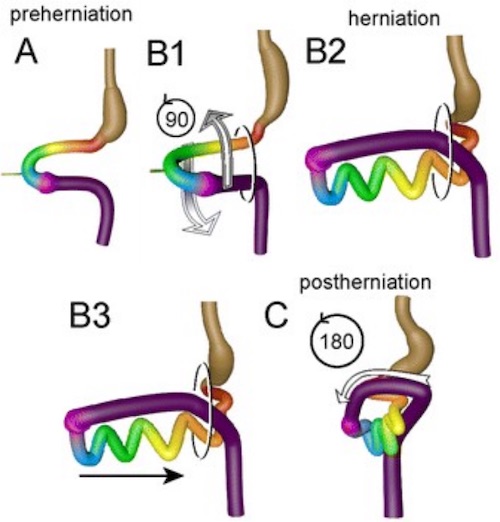
Classic “En-Bloc Rotation” Model of Gut Morphogenesis: Midgut Herniates and Rotates 90-Degrees (B1), Forms Loops (B2), & Slides Back into the Abdomen (B3). The Midgut Then Rotates an Additional 180-Degrees to its Final Position (C). 1

Malrotation Causing Volvulus 2
Malrotation Causing Duodenal Obstruction 3

Malrotation on UGI 4
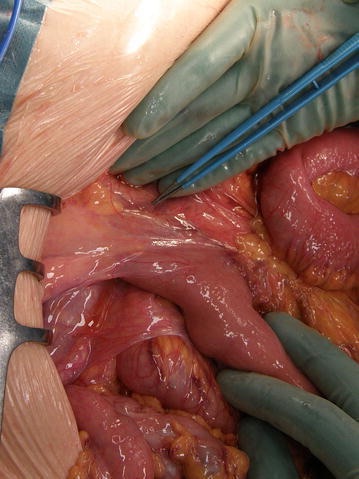
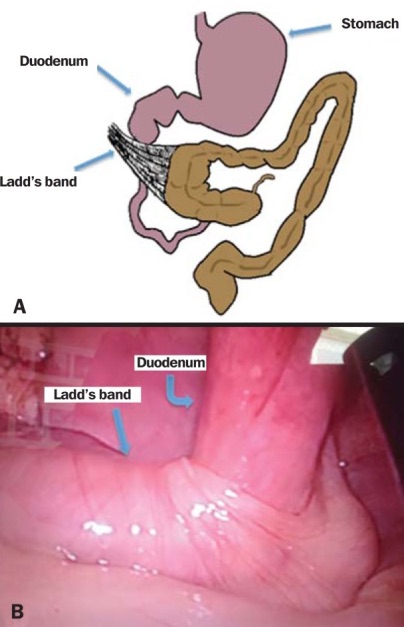
Ladds Bands 5