Definition: Loop of Bowel Invaginates/Telescopes into Itself
Segments:
Intussusceptum – Prolapsed Bowel
Intussuscipiens – Recipient Bowel
Most Common in Peds, Rare in Adults
Lead Points
Hypertrophied Peyer Patches (Viral Infection) – Most Common Lead Point in Peds
Meckel’s Diverticulum – Most Common Pathologic Lead Point in Peds
Cancer – Most Common Lead Point in Adults
Inspissated Stool of Cystic Fibrosis
Bowel Wall Hematoma
Idiopathic
Pediatric Postoperative Ileus
Classically After A Prolonged Laparotomy but Can Occur After Any Surgery, Even Nonabdominal Procedures
Most Common Site: Ileoileal
Intussusception 1
Location
Enteroenteric – Small Bowel into Small Bowel
Ileocolic – Terminal Ileum into Colon
The Most Common Site (90%)
Colocolic – Large Bowel into Large Bowel
Symptoms
Intermittent Abdominal Pain
Sausage-Shaped Abdominal Mass in Peds
Currant Jelly Stools (Blood & Mucous from Vascular Congestion)
SBO – Nausea, Vomiting & Obstipation
Diagnosis
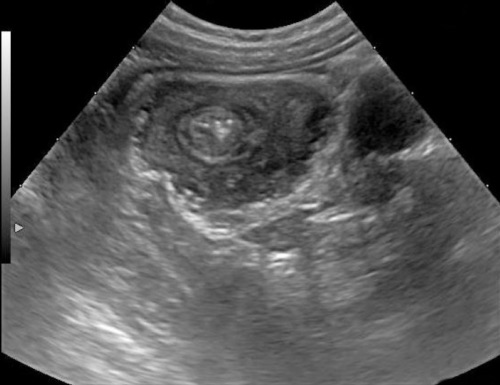
Peds: US (Target Sign)
Adults: CT
Intussusception on US 2
Intussusception on CT 3
Treatment – Pediatrics
Primary Treatment: Air-Contrast Enema to Reduce
Both Pneumatic (Air) or Hydrostatic (Saline/Contrast) are Acceptable
Max Pneumatic Pressure: 120 mm Hg
Max Barium Enema Column Height: 1 Meter/3 Feet
Do Not Attempt Air-Contrast Enema if After a GI Surgery – Will Require Operative Reduction
70-85% Success; 10-20% Recur
If Successful: Observe for 4 Hours & Discharge
If Fails: Repeat Enema
Can Repeat Multiple Times if Needed
Risk for Perforation with Radiographic Reduction (< 1%)
Perforation More Common in Intussuscipiens than the Intussusceptum
Risk Similar for Pneumatic & Hydrostatic
Increased Risk if Young (< 6 Months) & Long Duration of Symptoms (> 36 Hours)
Surgery:
Indications:
Hemodynamically Unstable
Peritonitis or Perforation
Complete Failure of Air-Contrast Enema
Procedure: Reduction & Resection of Any Necrotic Bowel
Reduction: Apply Pressure to Distal End (Intussuscipiens) & Milk
Do Not Apply Traction to the Proximal End
Treatment – Adults
Primary Treatment: Resection & Lymphadenectomy
*There is Some Newer Evidence that Not All Patients Require Surgery, Some Present with Frequent Intussusception that May be Due to Peristalsis without Lead Point – “Safe Answer” at this Time is Surgery
References
Joyce KM, Waters PS, Waldron RM, Khan I, Orosz ZS, Németh T, Barry K. Recurrent adult jejuno-jejunal intussusception due to inflammatory fibroid polyp – Vanek’s tumour: a case report. Diagn Pathol. 2014 Jun 27;9:127. (License: CC BY-4.0)
Zavras N, Tsilikas K, Vaos G. Chronic Intussusception Associated with Malrotation in a Child: A Variation of Waugh’s Syndrome? Case Rep Surg. 2016;2016:5638451. (License: CC BY-4.0)
Kee HM, Park JY, Yi DY, Lim IS. A Case of Intussusception with Acute Appendicitis. Pediatr Gastroenterol Hepatol Nutr. 2015 Jun;18(2):134-7. (License: CC BY-NC-3.0)