Exposure
- Divide Falciform Ligament – Visualize Superior or Lateral Aspects
- Divide Triangular Ligaments – Further Mobilize the Right/Left Lobes
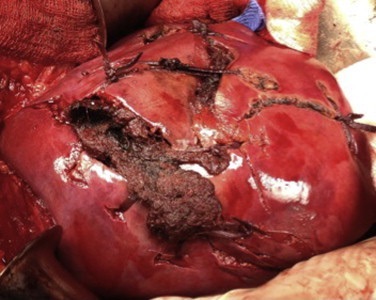
- If Stable Hematoma Noted Within Triangular Ligament: Do Not Enter
- Concern for Hepatic Vein or IVC Injury
Achieving Initial Surgical Hemostasis
- Initial: Manual Compression Until Resuscitated
- *Most Liver Bleeding is Venous
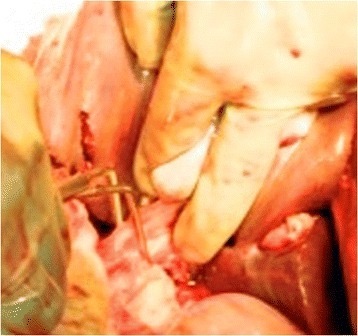
- If Significant Hemorrhage After Release: Pringle Maneuver
- 85% Success in Complex Injuries
- Up to 75 Minutes Without Adverse Sequelae
- Failure Raises Concern for Hepatic Vein/IVC Injury
- Options if Still Bleeding After Pringle Maneuver:
- Total Hepatic Isolation – Involves Pringle Maneuver, Infrahepatic IVC Occlusion & Suprahepatic IVC Occlusion
- Also Consider Supraceliac Aortic Occlusion – Abdominal Blood Flow Will Be Lost from Circulation Above the Diaphragm
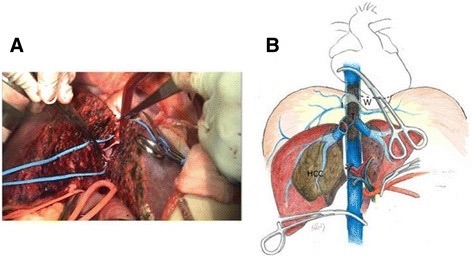
- Atriocaval (Schrock) Shunt
Atriocaval (Schrock) Shunt
- Consider for Retrohepatic Venous Injury
- Shunt from IVC to Right Atrium
- Technique:
- Pringle Maneuver
- Median Sternotomy
- Prepare Shunt
- Chest Tube – Cut a Hole 20 cm from the Nearest Drainage Hole
- Endotracheal Tube – Cut a Hole 17-18 cm from the Nearest Hole Past the Balloon
- Control Perihepatic IVC with Rumel Tourniquets:
- Control Suprarenal IVC (Omit Step if Using an ETT)
- Control Intrapericardial IVC
- Insert the Shunt Through a Right Atrial Incision
- Apply a Partially Occluding Clamp on the Right Atrial Appendage
- Place a Purse-String Suture
- Create an Incision Between the Purse-String
- Remove the Clamp
- Insert the Shunt Through the Incision
- Palpate the Tube terminating in the Correct Infrarenal Position
- All Shunt Holes Should Be Outside the Area of Vascular Isolation
- Secure all Purse-Strings, Tourniquets or Inflated Balloons