
Lymphedema; (Left) Left Leg, (Right) Right Arm 1

Lymphangiosarcoma 16 Years After Mastectomy 2
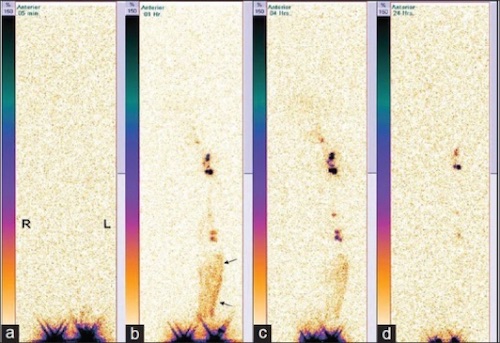
Serial Lymphoscintigraphy Showing Lymphedema ((a) Immediate, (b) 1h, (c) 4h, (d) 24h); RLE No Uptake in Lymph Nodes or Channels, LLE with Dermal Backflow (Arrows) 3

Lymphangitis After Bug Bites 4
Pelvic Lymphocele After Radical Cystectomy 5