di Summa PG, Yvon A, Larcher L, Raffoul W, Koch N. Propionibacterium avidum infection following breast reduction: high morbidity from a low-virulence pathogen. J Surg Case Rep. 2015 Feb 10;2015(2):rjv002. (License: CC BY-NC-4.0)
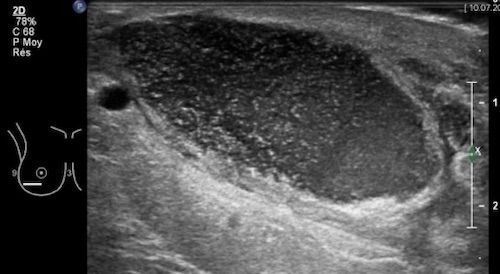
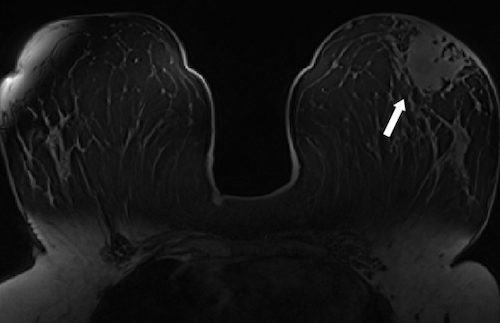
Bilal A, Badar Albadar F, Bashir Barlas N. Granulomatous Mastitis: Imaging of Temporal Evolution. Scientifica (Cairo). 2016;2016:3737528. (License: CC BY-4.0)