Management of Primary Lesion
- If Previously Diagnosed by Shave-Biopsy with Positive Deep Margin: Need Full Thickness Biopsy to Determine Depth
- Primary Treatment: Wide Local Excision
- Margins: Mn
- In Situ: 0.5-1.0 cm
- ≤ 1.0 mm Depth: 1.0 cm
- > 1.0 mm Depth: 1.0-2.0 cm
- > 2.0 mm Depth: 2.0 cm
- In General Length to Width Ratio of 3:1 Required to Allow Primary Closure
- Subungual Melanomas: Amputation of Distal Digit (1 cm Margin)
Management of Lymph Nodes
- Consider Systemic Immunotherapy for any Stage III Disease
- Clinically Palpable Lymph Nodes: FNA (Fine Needle Aspiration)
- Resect if Positive (Goal is to Clear, Not to Stage)
- Sentinel Lymph Node Biopsy (SLNB)
- Indications: ≥ T1b (≥ 0.8 mm or Ulcerating)
- Indications for Node Retrieval:
- Dye: All Nodes That Have Taken Up Dye
- Radiotracer: All Nodes with > 10% Highest Ex-Vivo Count
- Any Firm Node, Regardless of Dye/Radiotracer
- Most Commonly Sent for Permanent Pathology – Frozen Section Generally Abandoned Due to Low Sensitivity
- Completion Lymphadenectomy:
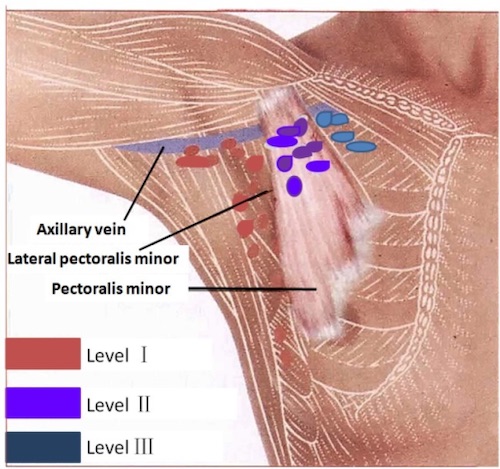
- Axillary Lymph Node Dissection (ALND)
- Indications: Positive SLNB or Axillary Nodes with No Primary
- Include Level III Nodes for Melanoma
- Groin Dissection
- Superficial Groin (Inguinofemoral) Dissection
- Indications: SLNB Positive
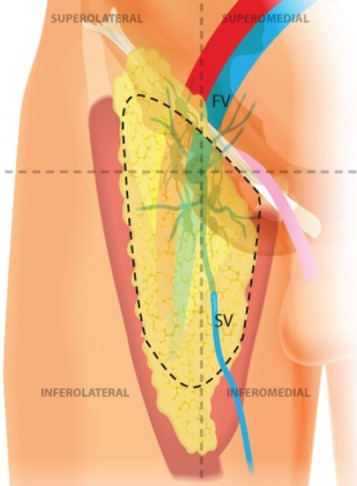
- Femoral Triangle Borders:
- Lateral: Sartorius
- Medial: Adductor Longus
- Superior: Inguinal Ligament
- Deep Inguinal (Iliac-Obturator) Dissection
- Indications: Cloquet’s LN Positive
- Cloquet’s LN – Within Femoral Canal (Bridge Between Superficial & Deep Nodal Basins)
- Procedure:
- Divide Inguinal Ligament Medially (Avoid Femoral Vessels)
- Start at Common Iliac Vessels and Extend Caudally
- Suture Inguinal Ligament to Lacunar Ligament to Close Femoral Canal
- Close Residual Defects with Mesh or Sartorius Flap
- If Sentinel LN+ May Consider US Observation:
- Observation with US & Completion LN Dissection Have Similar Melanoma-Specific Survival
- US Schedule:
- Every 4 Months for 2 Years
- Then Every 6 Months for 3 Years
- Then Annually
Management of Metastases
- Limited (Resectable): Systemic Therapy & Resect
- Disseminated (Unresectable): Systemic Therapy
Systemic Therapies
- Immunotherapy:
- Nivolumab: Monoclonal Antibody (mAb) Against PD-1
- Pembrolizumab: Monoclonal Antibody (mAb) Against PD-1
- Ipilimumab: Monoclonal Antibody (mAb) Against CTLA-4
- Molecular Targeted Therapy for BRAF V600-Activating Mutations:
- Dabrafenib (BRAF Inhibitor) & Trametinib (MEK Inhibitor)
- Vemurafenib (BRAF Inhibitor) & Cobimetinib (MEK Inhibitor)
- Encorafenib (BRAF Inhibitor) & Binimetinib (MEK Inhibitor)