Most Common Initial Manifestation
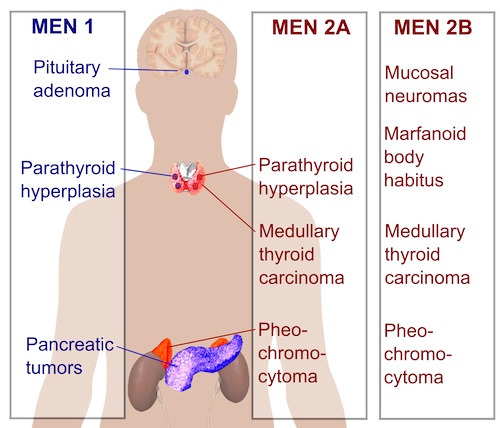
- MEN I: Primary Hyperparathyroidism
- MEN IIA/IIB: Medullary Thyroid Carcinoma
Most Common Cause of Death
- MEN I: Nonfunctional Pancreatic Tumor Malignancy
- MEN IIA/IIB: Medullary Thyroid Carcinoma
- MEN IIA Risk: 9.7%
- MEN IIB Risk: 50%
Screening Tests
- Indications:
- All Diagnosed Patients Should be Screened for Other Associated Tumors
- All First/Second Degree Family Members Should be Screened for Other Associated Tumors & Gene Mutations
- MEN I:
- Metabolic Panel (Including Calcium)
- Gastrin Level
- Prolactin Level
- MEN IIA/IIB:
- Metabolic Panel (Including Calcium) – Not Needed for Type IIB
- Calcitonin Level & Thyroid US
- Plasma Metanephrines
First Manifestation to Surgically Correct if Multiple are Concurrent
- MEN I: Primary Hyperparathyroidism
- MEN IIA/IIB: Pheochromocytoma
Prophylactic Thyroidectomy in MEN IIA/IIB
- MEN IIA:
- Low/Moderate-Risk Mutations: Start Clinical Monitoring by 3-5 Years of Age
- High-Risk Mutations: Thyroidectomy Before Age 5 Years
- MEN IIB: Thyroidectomy in First Year of Life Mn