
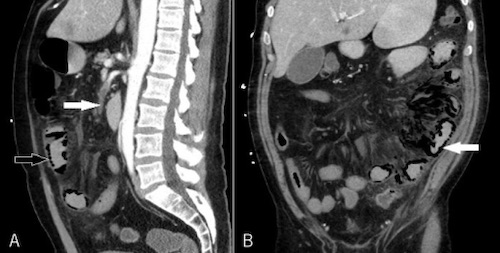
Necrotic Bowel from Mesenteric Ischemia 1
Mesenteric Ischemia with Embolism on CTA 2
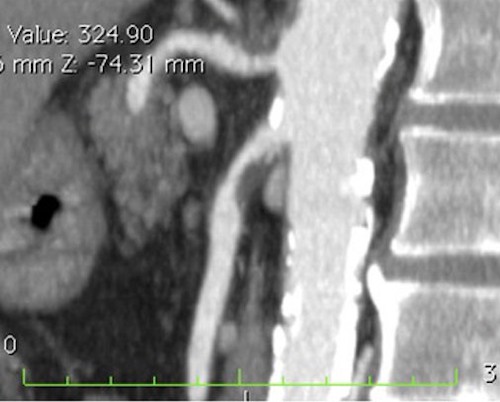
Mesenteric Ischemia from SMA Stenosis on CTA 3
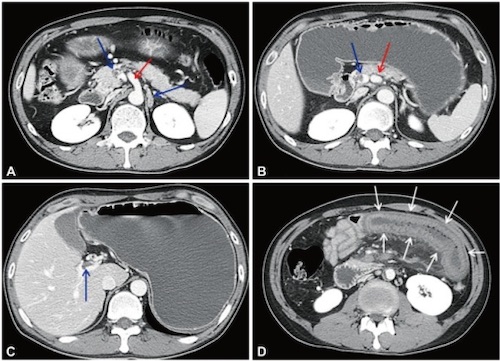
Mesenteric Venous Thrombosis on CTA – SMV Thrombus (Blue Arrows), Intact SMA (Red Arrows), Edematous Jejunum (White Arrows) 4
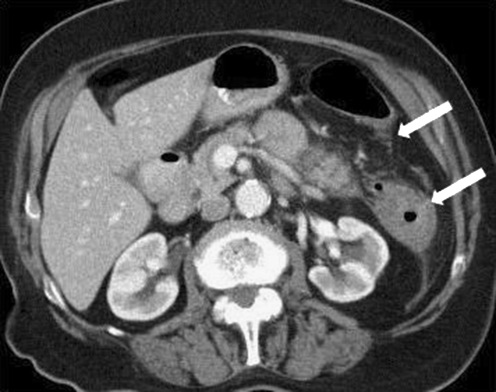
NOMI with Ischemia at Griffith’s Point 5
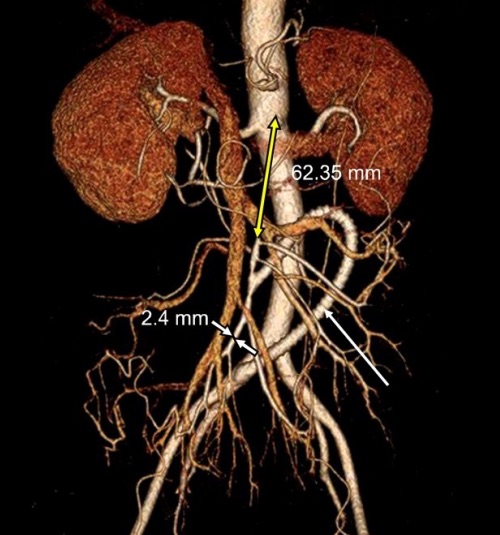
SMA Bypass with C-Loop Graft 6