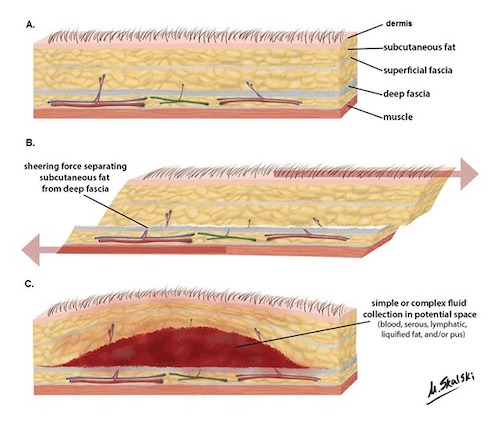
Morel-Lavallee Lesion – Mechanism of Injury 1
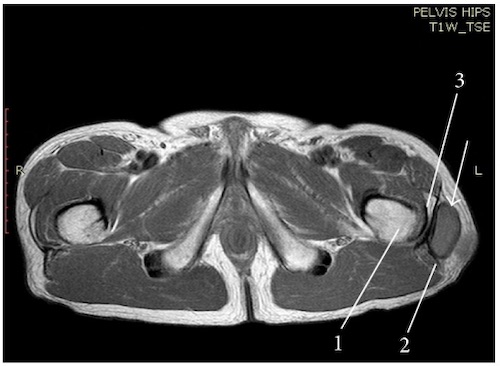
Morel-Lavallee Lesion on MRI 2

Morel-Lavallee Lesion – Skin Necrosis on Day #4 3
Morel-Lavallee Lesion – Mechanism of Injury 1
Morel-Lavallee Lesion on MRI 2
Morel-Lavallee Lesion – Skin Necrosis on Day #4 3