
NSTI of Abdominal Wall 1

Necrotizing Fasciitis 2

Fournier’s Gangrene 3

Soft Tissue Gas on XR
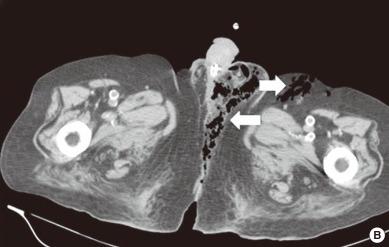
Fournier Gangrene on CT 4
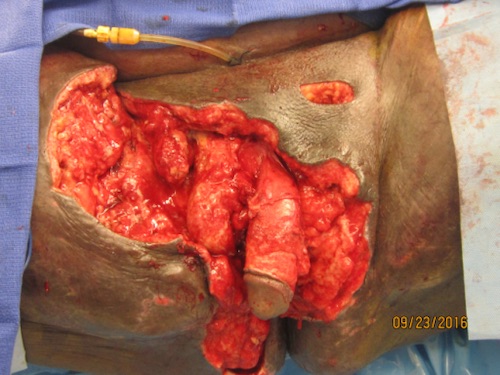
Aggressive Surgical Debridement 5
NSTI of Abdominal Wall 1
Necrotizing Fasciitis 2
Fournier’s Gangrene 3
Soft Tissue Gas on XR
Fournier Gangrene on CT 4
Aggressive Surgical Debridement 5