
FES Petechial Rash 1
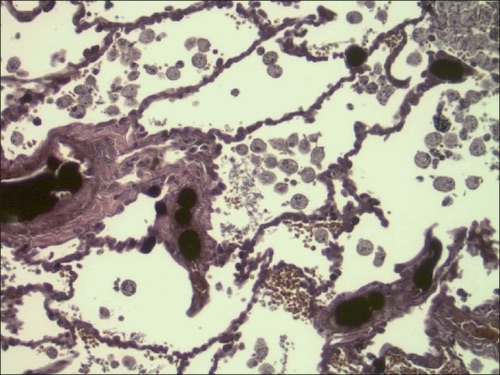
Lung Section with Extensive Fat Embolism and Fat Droplets in Alveolar Macrophages 2
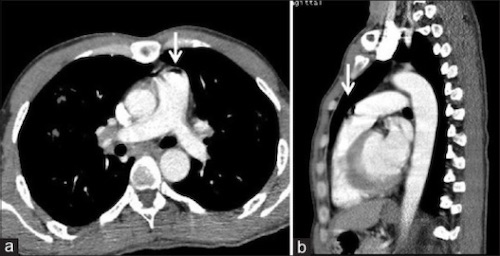
Air Embolism (Arrow) in Pulmonary Artery 3

Mill Wheel 1
FES Petechial Rash 1
Lung Section with Extensive Fat Embolism and Fat Droplets in Alveolar Macrophages 2
Air Embolism (Arrow) in Pulmonary Artery 3
Mill Wheel 1