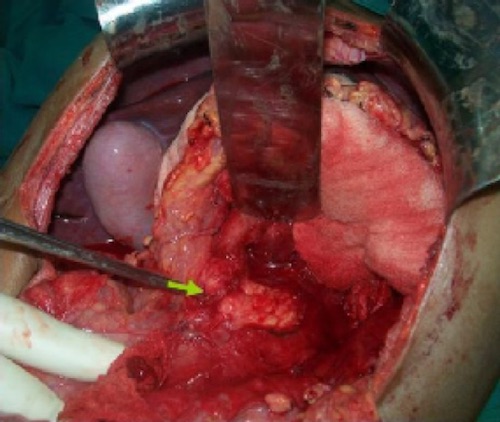
Pancreatic Neck Laceration 1
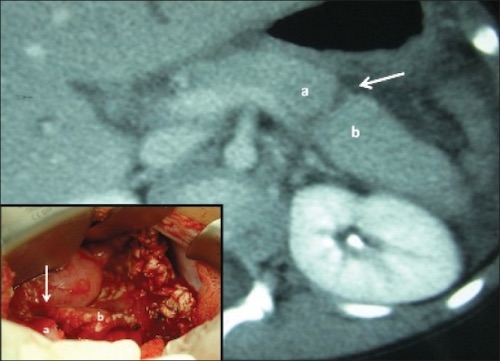
Distal Pancreas Laceration 2
![]()
Pancreatic Duct Transection MRCP 3

Distal Pancreatectomy & Splenectomy 4
Pancreatic Neck Laceration 1
Distal Pancreas Laceration 2
![]()
Pancreatic Duct Transection MRCP 3
Distal Pancreatectomy & Splenectomy 4