
Omphalocele
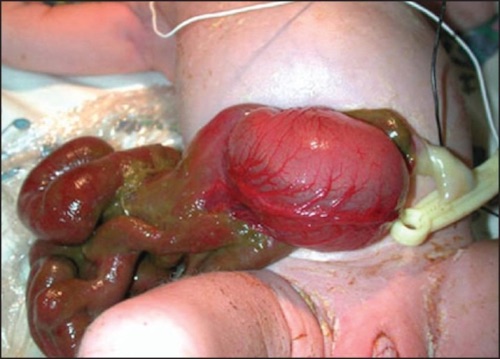
Gastroschisis 1

Gastroschisis Silo 2

Umbilical Cord Hernia Containing a Meckel’s Diverticulum 3

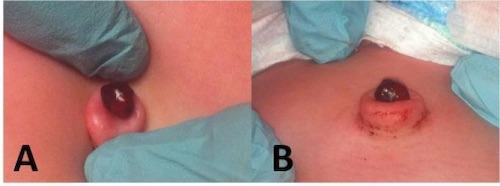
Patent Omphalomesenteric Duct, (A) Prolapsed Patent Duct, (B) Meconium Drainage from Patent Duct 4

Omphalitis 5
Umbilical Granuloma 6
Omphalocele
Gastroschisis 1
Gastroschisis Silo 2
Umbilical Cord Hernia Containing a Meckel’s Diverticulum 3
Patent Omphalomesenteric Duct, (A) Prolapsed Patent Duct, (B) Meconium Drainage from Patent Duct 4
Omphalitis 5
Umbilical Granuloma 6