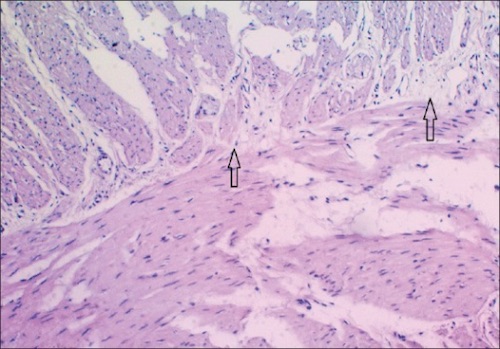
Hirschsprung Histology: No Myenteric Plexus Between the Two Muscle Layers 1
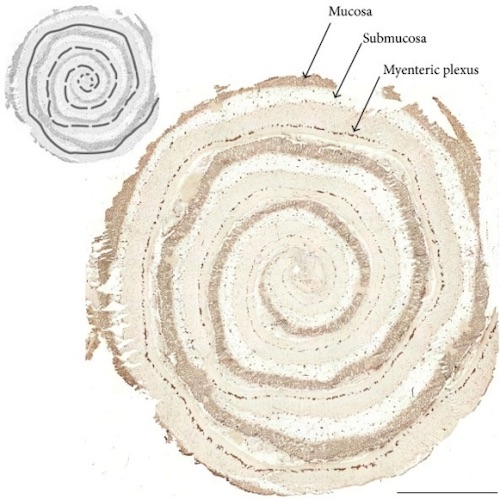
Hirschsprung Tissue “Swiss-Rolled”, Center is More Distal 2
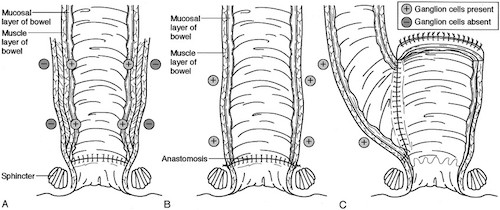
Pull-Through Procedures; (A) Soave, (B) Swenson, (C) Duhamel 3
Hirschsprung Histology: No Myenteric Plexus Between the Two Muscle Layers 1
Hirschsprung Tissue “Swiss-Rolled”, Center is More Distal 2
Pull-Through Procedures; (A) Soave, (B) Swenson, (C) Duhamel 3