No Axonal Recovery: Surgery & Monitor for Action Potentials Across Lesion
Action Potentials Recorded (Axonotmesis) – Conservative Treatment
No Action Potentials Recorded (Neurotmesis) – Surgical Repair
Open Injury
Lesion in Continuity: Conservative Management
Lesion in Discontinuity:
Laceration: Immediate Repair
Blunt Transection: Early Repair (2-4 Weeks)
Allow Decreased Inflammation
*May Require Radial/Sural Nerve Graft if Contracted
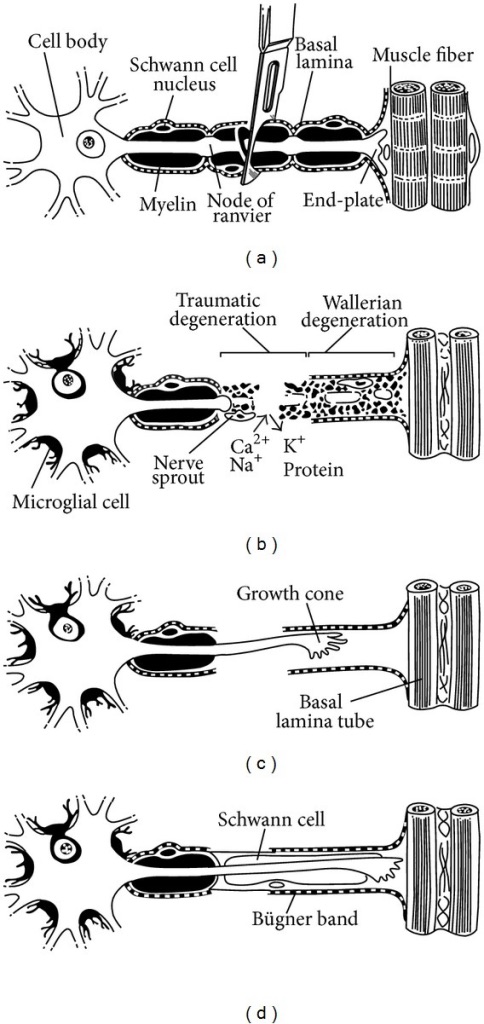
Peripheral Nerve Degeneration & Regeneration 1
Vascularized Sural Nerve Graft 1
References
Grinsell D, Keating CP. Peripheral nerve reconstruction after injury: a review of clinical and experimental therapies. Biomed Res Int. 2014;2014:698256. (License: CC BY-3.0)